

Validation of the RayStation Monte Carlo dose calculation algorithm using realistic animal tissue phantoms
- PMID: 31541536
- PMCID: PMC6806482
- DOI: 10.1002/acm2.12733
Validation of the RayStation Monte Carlo dose calculation algorithm using realistic animal tissue phantoms
Abstract
Purpose: The aim of this study is to validate the RayStation Monte Carlo (MC) dose algorithm using animal tissue neck phantoms and a water breast phantom.
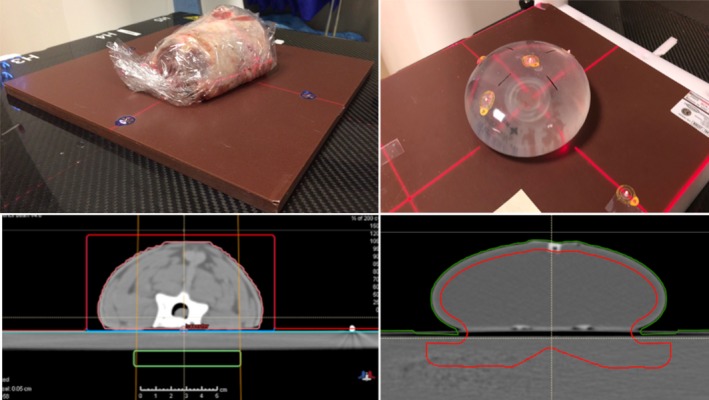
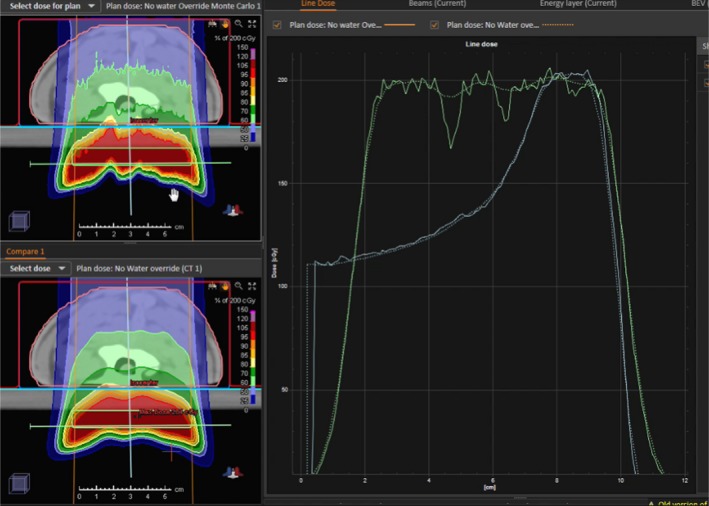
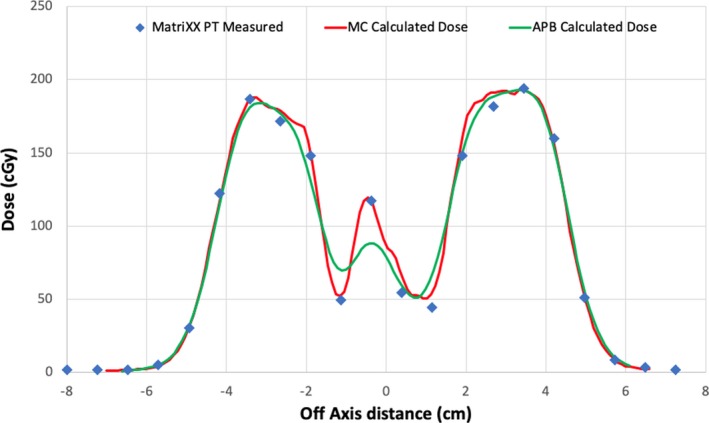
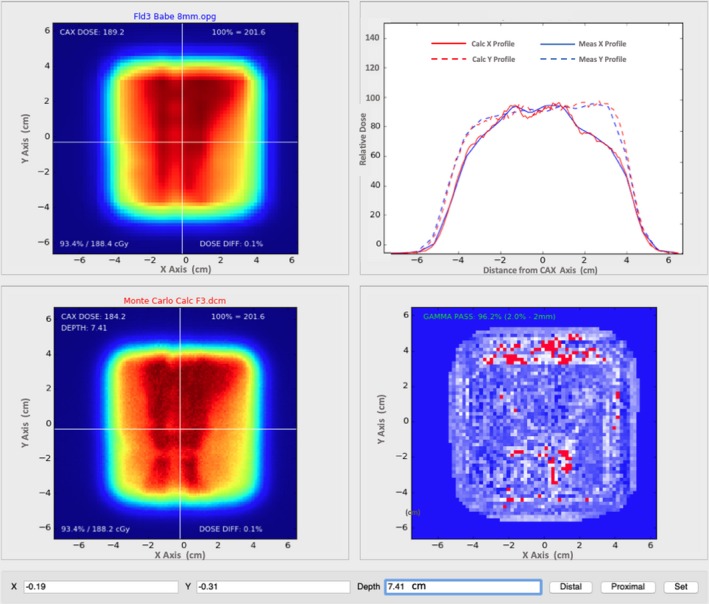
Methods: Three anthropomorphic phantoms were used in a clinical setting to test the RayStation MC dose algorithm. We used two real animal necks that were cut to a workable shape while frozen and then thawed before being CT scanned. Secondly, we made a patient breast phantom using a breast prosthesis filled with water and placed on a flat surface. Dose distributions in the animal and breast phantoms were measured using the MatriXX PT device.
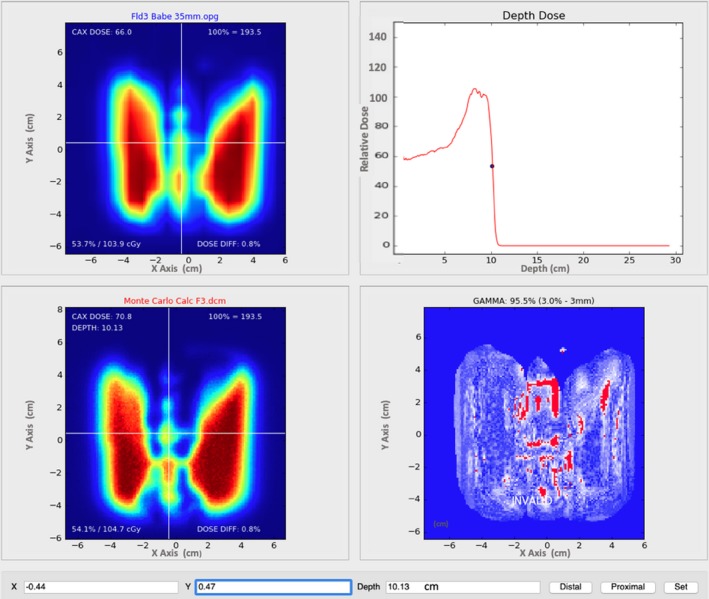
Results: The measured doses to the neck and breast phantoms compared exceptionally well with doses calculated by the analytical pencil beam (APB) and MC algorithms. The comparisons between APB and MC dose calculations and MatriXX PT measurements yielded an average depth difference for best gamma agreement of <1 mm for the neck phantoms. For the breast phantom better average gamma pass rates between measured and calculated dose distributions were observed for the MC than for the APB algorithms.
Conclusions: The MC dose calculations are more accurate than the APB calculations for the static phantoms conditions we evaluated, especially in areas where significant inhomogeneous interfaces are traversed by the beam.
Keywords: Monte Carlo; analytical dose algorithms; pencil beam scanning; proton therapy; spot scanning.
© 2019 The Authors. Journal of Applied Clinical Medical Physics published by Wiley Periodicals, Inc. on behalf of American Association of Physicists in Medicine.
Conflict of interest statement
The authors have no relevant conflict of interest to disclose.
Figures
References
-
- Durante MORLJ. Charged‐particle therapy in cancer: clinical uses and future perspectives. Nat Rev: Clin Oncol. 2017;14:483–495. - PubMed
-
- Particle Therapy Co‐Operative Group . Particle therapy facilities in operation. Particle Therapy Co‐Operative Group. 2018. Available at: https://ptcog.ch/index.php/facilities‐in‐operation. Accessed November 29, 2018.
-
- Schreuder AN, Hedrick SG, Renegar JR, et al. A review of proton radiation therapy and the path to widespread clinical adoption. Med Phys Int J. 2016;4:35–46.
-
- Bortfeld TR, Loeffler JS. Three ways to make proton therapy affordable. Nature. 2017;549:451–453. - PubMed
-
- Löf J. First PBS/IMPT Proton Treatments with RayStation. 2014. Available at: https://www.raysearchlabs.com/media/press‐old/?year=2014&cisionid =1629464. Accessed November 26, 2018.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
