

Review
doi: 10.1016/j.ipej.2019.09.004.
Epub 2019 Sep 18.
Neonatal supraventricular tachycardia
Affiliations
- PMID: 31541680
- PMCID: PMC6904811
- DOI: 10.1016/j.ipej.2019.09.004
Item in Clipboard
Review
Neonatal supraventricular tachycardia
Indian Pacing Electrophysiol J.
2019 Nov-Dec.
Abstract
Supraventricular tachycardia (SVT) is one of the most common conditions requiring emergency cardiac care in neonates. Atrioventricular reentrant tachycardia utilizing an atrioventricular bypass tract is the most common form of SVT presenting in the neonatal period. There is high likelihood for spontaneous resolution for most of the common arrhythmia substrates in infancy. Pharmacological agents remain as the primary therapy for neonates.
Keywords: Neonate; Supraventricular tachycardia.
Production and hosting by Elsevier B.V.
Figures

Common reentrant supraventricular tachycardias presenting as narrow QRS-complex tachycardia. The direction of the arrows in each case indicates the direction of propagation within reentrant circuits. The slow pathways within the circuit are represented by ‘wavy’ arrows. The lower panel illustrates the presence (“manifest” with ventricular preexcitation) and absence (“concealed” without ventricular preexcitation) of antegrade conduction via atrioventricular bypass tract in sinus rhythm which in turn is a substrate for orthrodromic atrioventricular reentrant tachycardia. Note that the ventricle is not primarily a part of the reentrant circuit in atrial flutter, atrial fibrillation and atrioventricular nodal reentrant tachycardia. AVN, Atrioventricular node; AV BT, Atrioventricular bypass tract; HB, His bundle.
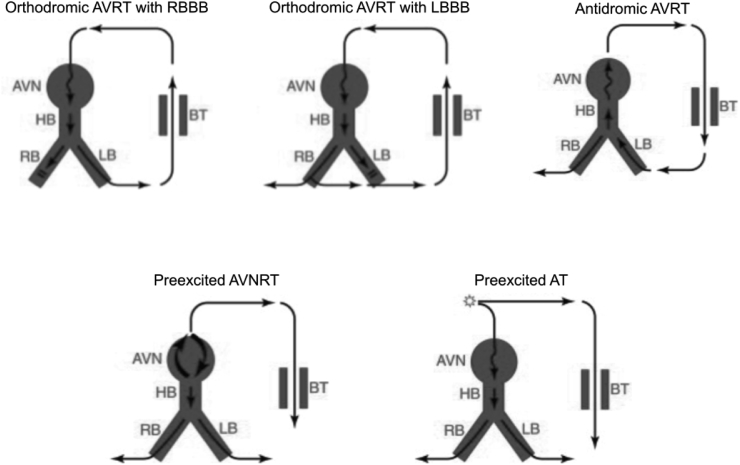
Common reentrant supraventricular tachycardias presenting as wide QRS-complex tachycardia. The direction of the arrows in each case indicates the direction of propagation within reentrant circuits. The slow pathways within the circuit are represented by ‘wavy’ arrows. Preexcited SVT refers to supraventricular tachycardias where atrioventricular accessory pathways capable of antegrade conduction act only as bystanders and not part of the primary arrhythmia substrate. AVN, Atrioventricular node; AVRT, Atrioventricular reentrant tachycardia; AVNRT, Atrioventricular nodal reentrant tachycardia; BT, Bypass tract; HB, His bundle; LB, Left bundle branch; LBBB, Left bundle branch block; RB, Right bundle branch; RBBB, Right bundle branch block; SVT, supraventricular tachycardia.

Algorithm for analysis of tachyarrhythmia on surface electrocardiogram. A.Flutter, Atrial flutter; A.Fib, Atrial fibrillation; AT, Atrial tachycardia; Atyp.AVNRT, Atypical AVNRT; AV, atrioventricular; BBB, Bundle branch block; AVRT, Atrioventricular reentrant tachycardia; AVNRT, Atrioventricular nodal reentrant tachycardia; IART, Intra-atrial reentrant tachycardia; JET, Junctional ectopic tachycardia; MAT, Multifocal atrial tachycardia; Orthodrom. AVRT, Orthodromic atrioventricular reentrant tachycardia; PJRT, Permanent Junctional Reciprocating Tachycardia; RP interval, measured from onset of QRS complex to onset of subsequent P wave on ECG; SVT, Supraventricular tachycardia; VT, Ventricular tachycardia; WPW, Wolff-Parkinson-White syndrome.

Three-day-old neonate presenting with permanent junctional reciprocating tachycardia (PJRT). Initial two beats are sinus beats followed by induction of PJRT. Note long-RP narrow QRS complex supraventricular tachycardia with inverted P waves in inferior frontal leads (II, III, aVF).

Case 1: ECG characteristics: ‘Narrow QRS complex’, 1:1 AV ratio, short RP interval (∼80 ms), and stable cycle length consistent with orthodromic atrioventricular reentrant tachycardia. Case 2: Short runs of nonsustained tachycardia shown. ‘S’ represents sinus beats. ‘A’ represents tachycardia beats. ECG characteristics: ‘Narrow QRS complex tachycardia with 1:1 AV ratio and long RP interval. Differential diagnosis includes Atrial tachycardia and Permanent Junctional Reciprocating Tachycardia (a form of orthodromic atrioventricular tachycardia utilizing a slowly conducting decremental retrograde only AV bypass tract, often presenting as incessant tachycardia). Case 3: ECG characteristics: ‘Narrow QRS complex’, <1:1 AV ratio, variable cycle length consistent with junctional ectopic tachycardia. Case 4: Top panel shows narrow QRS complex tachycardia with >1:1 AV ratio recorded at 25 mm/s. Bottom panel shows the same tachycardia recorded at 50 mm/s. Adenosine administered accentuates AV block and makes the atrial flutter waves easily visible. AV, atrioventricular.
References
-
- Lau E.W. Infraatrial supraventricular tachycardias: mechanisms, diagnosis, and management. Pacing Clin Electrophysiol. 2008;31:490–498. - PubMed
-
- Geggel R.L. Conditions leading to pediatric cardiology consultation in a tertiary academic hospital. Pediatrics. 2004;114:e409–e417. - PubMed
-
- Garson A., Gillette P.C., McNamara D.G. Supraventricular tachycardia in children: clinical features, response to treatment, and long-term follow-up in 217 patients. J Pediatr. 1981;98:875–882. - PubMed
-
- Lundberg A. Paroxysmal tachycardia in infancy. A clinical and experimental study. Acta Paediatr. 1963;52:192–195. - PubMed
-
- Nadas A.S., Daeschner C.W., Roth A., Blumenthal S.L. Paroxysmal tachycardia in infants and children; study of 41 cases. Pediatrics. 1952;9:167–181. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
