

Understanding neurodegeneration after traumatic brain injury: from mechanisms to clinical trials in dementia
- PMID: 31542723
- PMCID: PMC6860906
- DOI: 10.1136/jnnp-2017-317557
Understanding neurodegeneration after traumatic brain injury: from mechanisms to clinical trials in dementia
Abstract
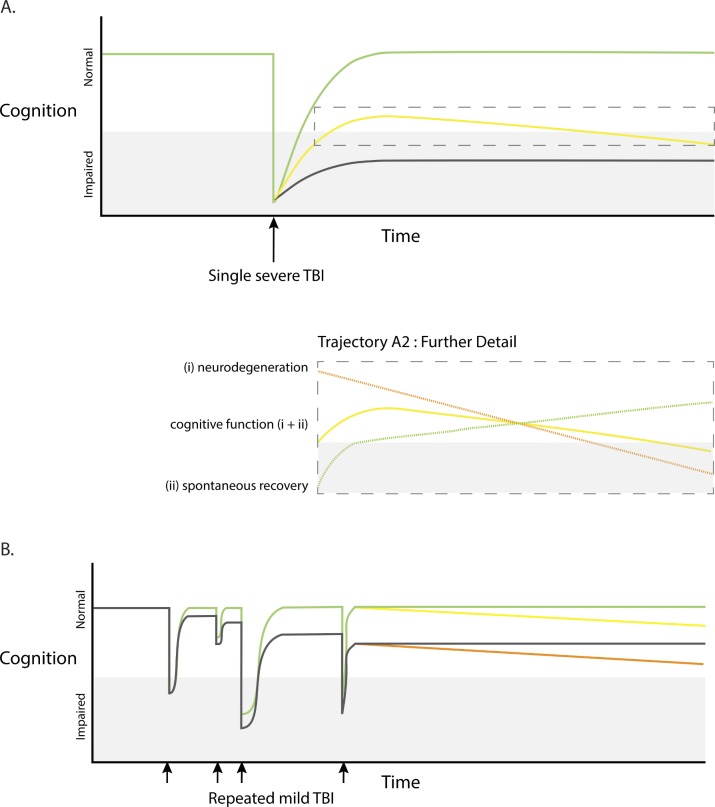
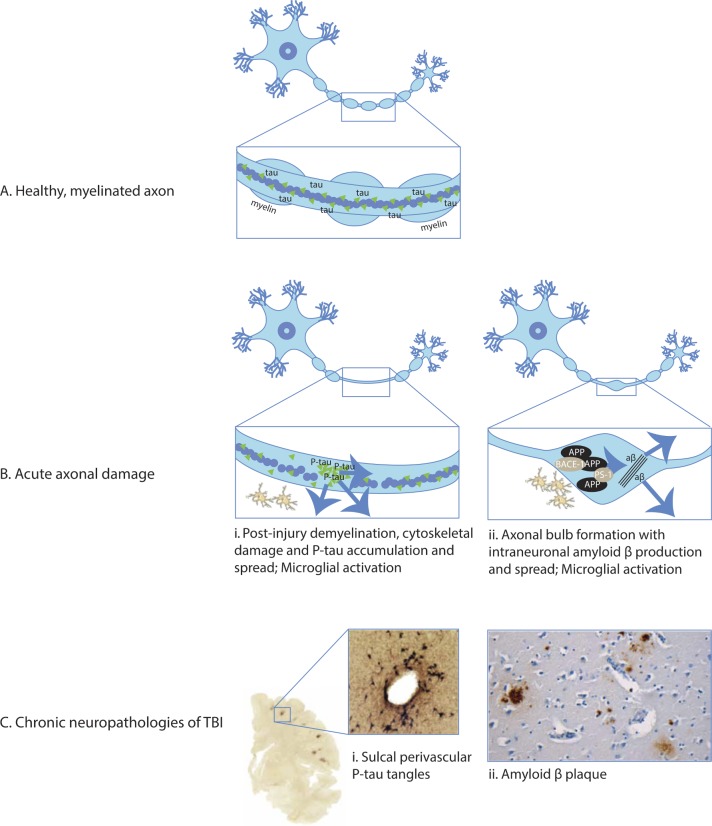
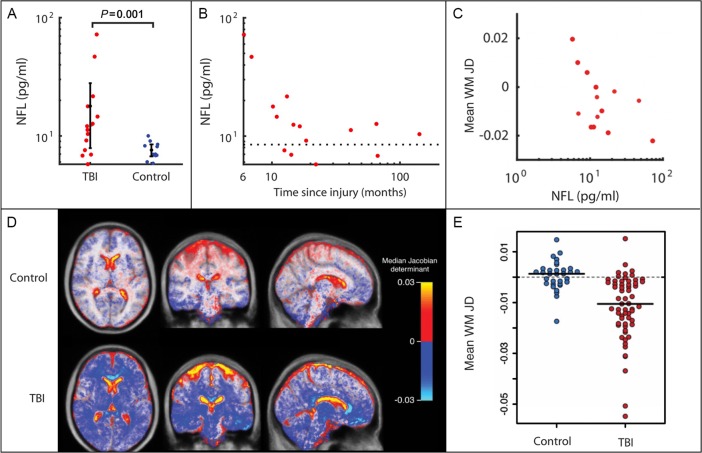
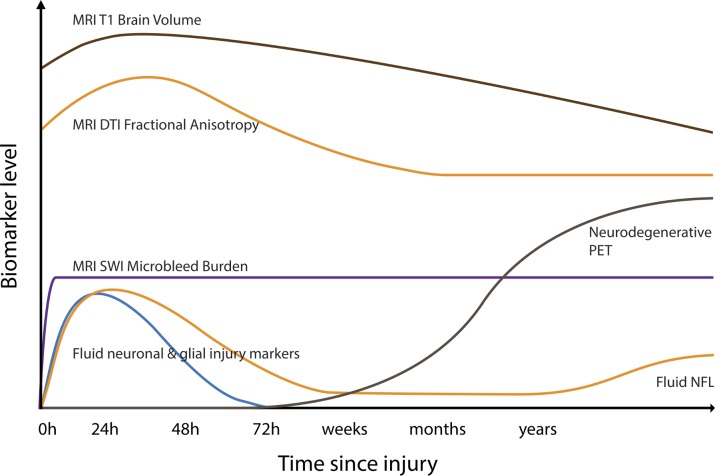
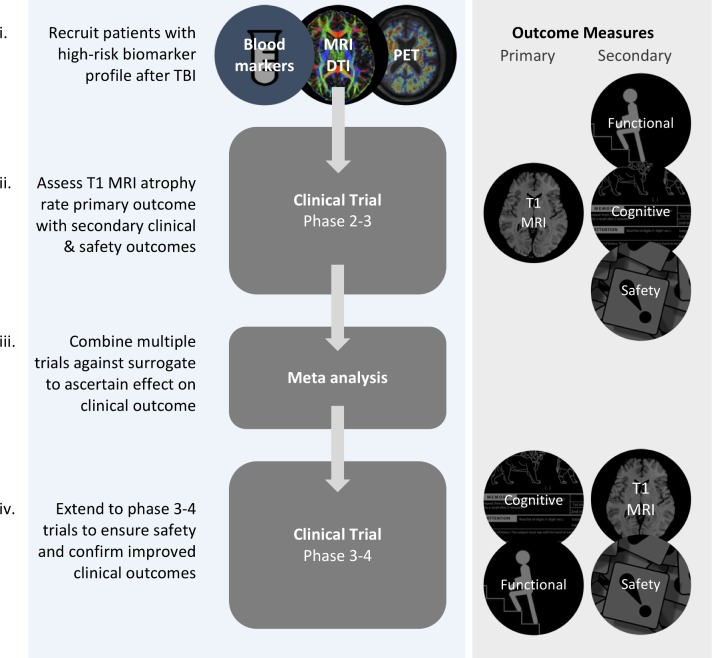
Traumatic brain injury (TBI) leads to increased rates of dementia, including Alzheimer's disease. The mechanisms by which trauma can trigger neurodegeneration are increasingly understood. For example, diffuse axonal injury is implicated in disrupting microtubule function, providing the potential context for pathologies of tau and amyloid to develop. The neuropathology of post-traumatic dementias is increasingly well characterised, with recent work focusing on chronic traumatic encephalopathy (CTE). However, clinical diagnosis of post-traumatic dementia is problematic. It is often difficult to disentangle the direct effects of TBI from those produced by progressive neurodegeneration or other post-traumatic sequelae such as psychiatric impairment. CTE can only be confidently identified at postmortem and patients are often confused and anxious about the most likely cause of their post-traumatic problems. A new approach to the assessment of the long-term effects of TBI is needed. Accurate methods are available for the investigation of other neurodegenerative conditions. These should be systematically employed in TBI. MRI and positron emission tomography neuroimaging provide biomarkers of neurodegeneration which may be of particular use in the postinjury setting. Brain atrophy is a key measure of disease progression and can be used to accurately quantify neuronal loss. Fluid biomarkers such as neurofilament light can complement neuroimaging, representing sensitive potential methods to track neurodegenerative processes that develop after TBI. These biomarkers could characterise endophenotypes associated with distinct types of post-traumatic neurodegeneration. In addition, they might profitably be used in clinical trials of neuroprotective and disease-modifying treatments, improving trial design by providing precise and sensitive measures of neuronal loss.
Keywords: acquired brain injury; cognition; dementia; image analysis; traumatic brain injury.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical