

Comparative thromboembolic risk in atrial fibrillation with and without a secondary precipitant-Danish nationwide cohort study
- PMID: 31542739
- PMCID: PMC6756362
- DOI: 10.1136/bmjopen-2018-028468
Comparative thromboembolic risk in atrial fibrillation with and without a secondary precipitant-Danish nationwide cohort study
Abstract
Objectives: We compared long-term outcomes in patients with atrial fibrillation (AF) with and without a secondary precipitant.
Design and setting: Retrospective cohort study based on Danish nationwide registries.
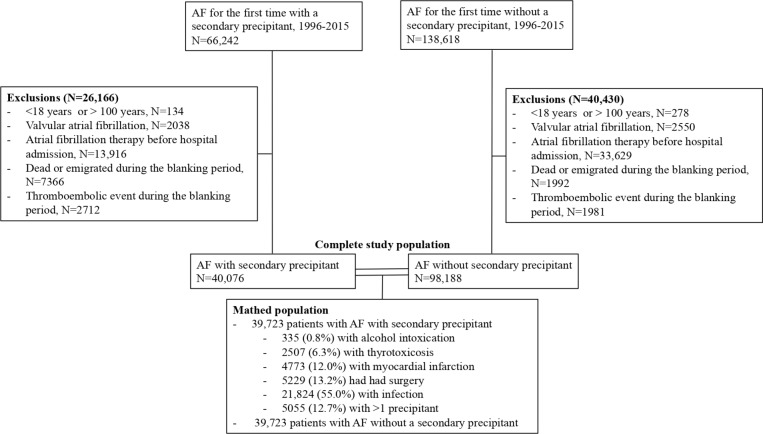
Participants: Patients with AF with and without secondary precipitants (1996-2015) were matched 1:1 according to age, sex, calendar year, CHA2DS2-VASc score and oral anticoagulation therapy (OAC), resulting in a cohort of 39 723 patients with AF with a secondary precipitant and the same number of patients with AF without a secondary precipitant. Secondary precipitants included alcohol intoxication, thyrotoxicosis, myocardial infarction, surgery and infection in conjunction with AF.
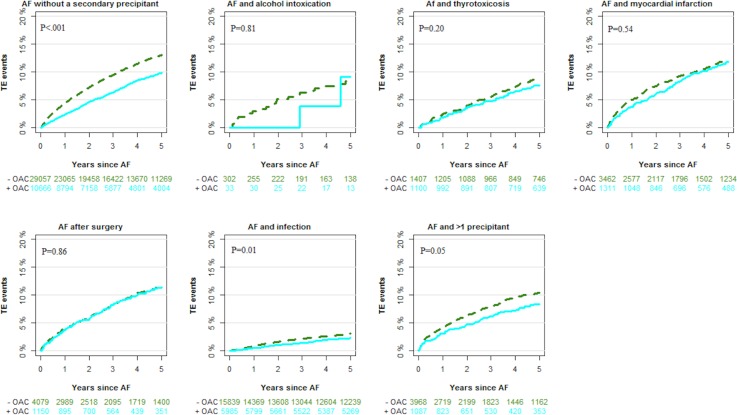
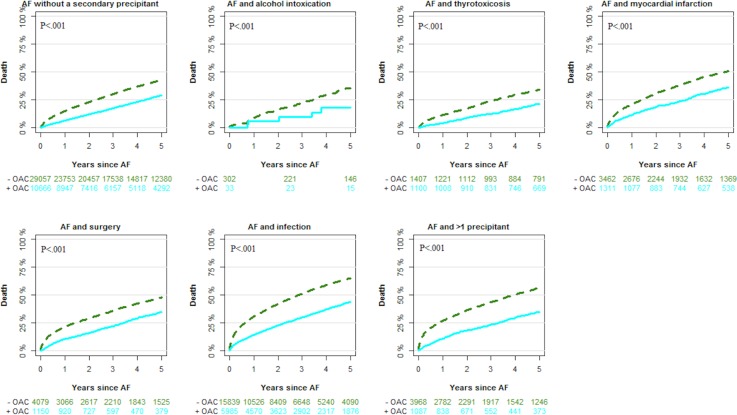
Primary and secondary outcomes: The primary outcome in this study was thromboembolic events. Secondary outcomes included AF rehospitalisation and death. Long-term risks of outcomes were examined by multivariable Cox regression analysis.
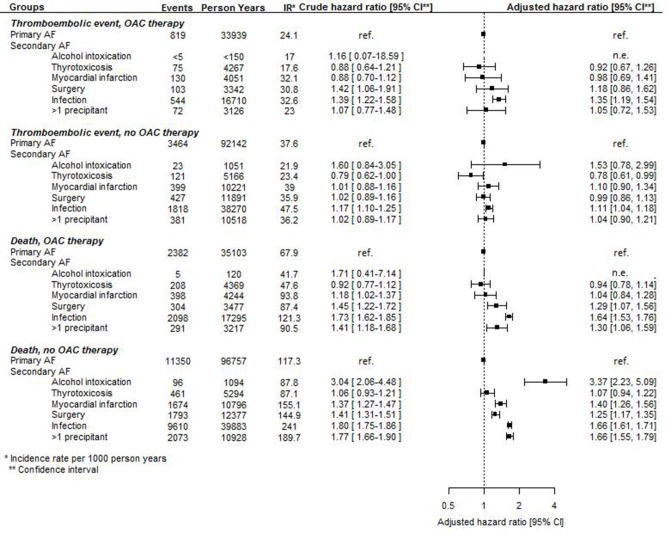
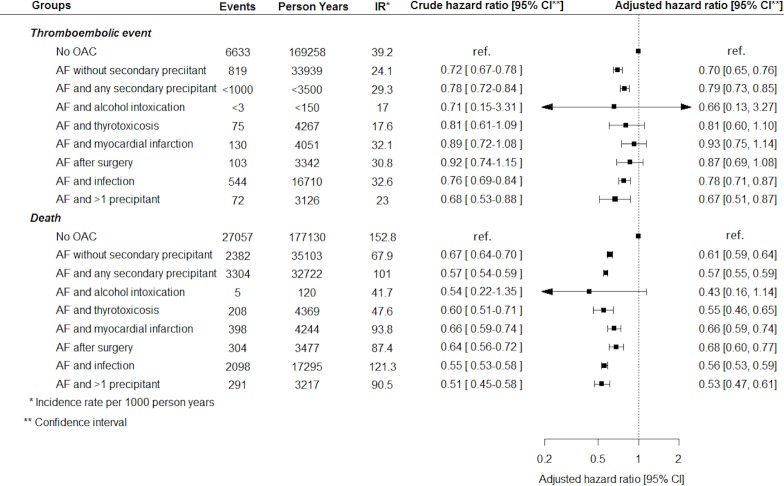
Results: The most common precipitants were infection (55.0%), surgery (13.2%) and myocardial infarction (12.0%). The 5-year absolute risk of thromboembolic events (taking death into account as a competing risk) in patients with AF grouped according to secondary precipitants were 8.3% (alcohol intoxication), 8.5% (thyrotoxicosis), 12.1% (myocardial infarction), 11.6% (surgery), 12.2% (infection), 10.1% (>1 precipitant) and 12.3% (no secondary precipitant). In the multivariable analyses, AF with a secondary precipitant was associated with the same or an even higher thromboembolic risk than AF without a secondary precipitant. One exception was patients with AF and thyrotoxicosis: those not initiated on OAC therapy carried a lower thromboembolic risk the first year of follow-up than matched patients with AF without a secondary precipitant and no OAC therapy.
Conclusions: In general, AF with a secondary precipitant was associated with the same thromboembolic risk as AF without a secondary precipitant. Consequently, this study highlights the need for more research regarding the long-term management of patients with AF associated with a secondary precipitant.
Keywords: recurrence; reversible atrial fibrillation; secondary precipitant.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: AG: none. TK: consultant fees from BMS, Astra Zeneca, Roche, Boehringer-Ingelheim, Bayer, MSD. JBO: speaker for Bristol-Myers Squibb, Boehringer Ingelheim, Bayer, and AstraZeneca. Consultant for Boehringer Ingelheim and Novo Nordisk. Funding for research from Bristol-Myers Squibb and The Capital Region of Denmark, Foundation for Health Research. ANB: none. JHB: none. GHG: research grants from Bayer, Bristol-Myers Squibb, AstraZeneca and Boehring Ingelheim. CT-P: consultant fees and research funding from Bayer and Biotronic. LK: none. ELF: has previously received research funding from Janssen and Janssen and Bristol-Myers Squibb.
Figures
References
-
- Fuster V, Rydén LE, Cannom DS, et al. 2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: a report of the American College of cardiology Foundation/American heart association Task force on practice guidelines. Circulation 2011;123:e269–367. 10.1161/CIR.0b013e318214876d - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical