

Observational retrospective study of the association of initial healthcare provider for new-onset low back pain with early and long-term opioid use
- PMID: 31542740
- PMCID: PMC6756340
- DOI: 10.1136/bmjopen-2018-028633
Observational retrospective study of the association of initial healthcare provider for new-onset low back pain with early and long-term opioid use
Erratum in
-
Correction: Observational retrospective study of the association of initial healthcare provider for new-onset low back pain with early and long-term opioid use.BMJ Open. 2020 Jan 10;10(1):e028633corr1. doi: 10.1136/bmjopen-2018-028633corr1. BMJ Open. 2020. PMID: 31924645 Free PMC article. No abstract available.
Abstract
Objective: This study examined the association of initial provider treatment with early and long-term opioid use in a national sample of patients with new-onset low back pain (LBP).
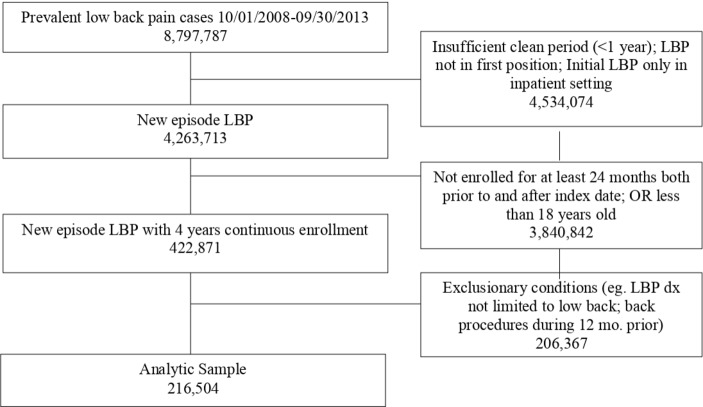
Design: A retrospective cohort study of patients with new-onset LBP from 2008 to 2013.
Setting: The study evaluated outpatient and inpatient claims from patient visits, pharmacy claims and inpatient and outpatient procedures with initial providers seen for new-onset LBP.
Participants: 216 504 individuals aged 18 years or older across the USA who were diagnosed with new-onset LBP and were opioid-naïve were included. Participants had commercial or Medicare Advantage insurance.
Exposures: The primary independent variable is type of initial healthcare provider including physicians and conservative therapists (physical therapists, chiropractors, acupuncturists).
Main outcome measures: Short-term opioid use (within 30 days of the index visit) following new LBP visit and long-term opioid use (starting within 60 days of the index date and either 120 or more days' supply of opioids over 12 months, or 90 days or more supply of opioids and 10 or more opioid prescriptions over 12 months).
Results: Short-term use of opioids was 22%. Patients who received initial treatment from chiropractors or physical therapists had decreased odds of short-term and long-term opioid use compared with those who received initial treatment from primary care physicians (PCPs) (adjusted OR (AOR) (95% CI) 0.10 (0.09 to 0.10) and 0.15 (0.13 to 0.17), respectively). Compared with PCP visits, initial chiropractic and physical therapy also were associated with decreased odds of long-term opioid use in a propensity score matched sample (AOR (95% CI) 0.21 (0.16 to 0.27) and 0.29 (0.12 to 0.69), respectively).
Conclusions: Initial visits to chiropractors or physical therapists is associated with substantially decreased early and long-term use of opioids. Incentivising use of conservative therapists may be a strategy to reduce risks of early and long-term opioid use.
Keywords: Back pain; Opioid use; PAIN MANAGEMENT; opioid.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: Drs OA, DS and DE work for OptumLabs but do not have any competing interests to report. This study was commissioned by OptumLabs and the American Physical Therapy Association (APTA). The funders provided comments on the production of the manuscript. The primary author, Dr LEK Professor at Boston University, had final editorial comment on the manuscript.
Figures
References
-
- Hughes A, Williams M, Lipari R. Prescription drug use and misuse in the United States: results from the 2015 national survey on drug use and health, 2016.
-
- Opioid Overdose [Internet] Centers for disease control and prevention. centers for disease control and prevention, 2017. Available: https://www.cdc.gov/drugoverdose/data/statedeaths.html [Accessed cited 6 Nov 2018].
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous