

Evaluating the effectiveness of the NHS Health Check programme in South England: a quasi-randomised controlled trial
- PMID: 31542745
- PMCID: PMC6756325
- DOI: 10.1136/bmjopen-2019-029420
Evaluating the effectiveness of the NHS Health Check programme in South England: a quasi-randomised controlled trial
Abstract
Objective: To evaluate uptake, risk factor detection and management from the National Health Service (NHS) Health Check (HC).
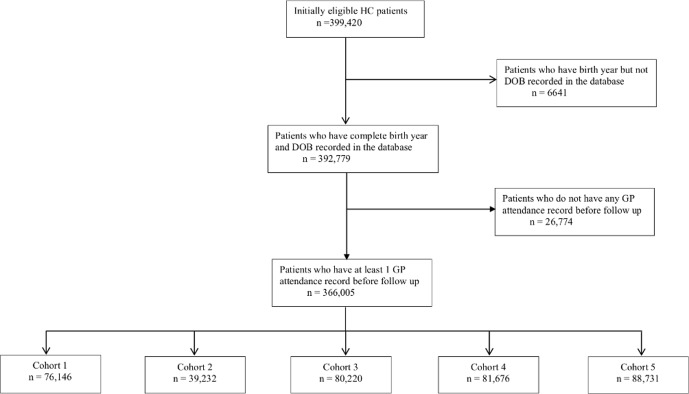
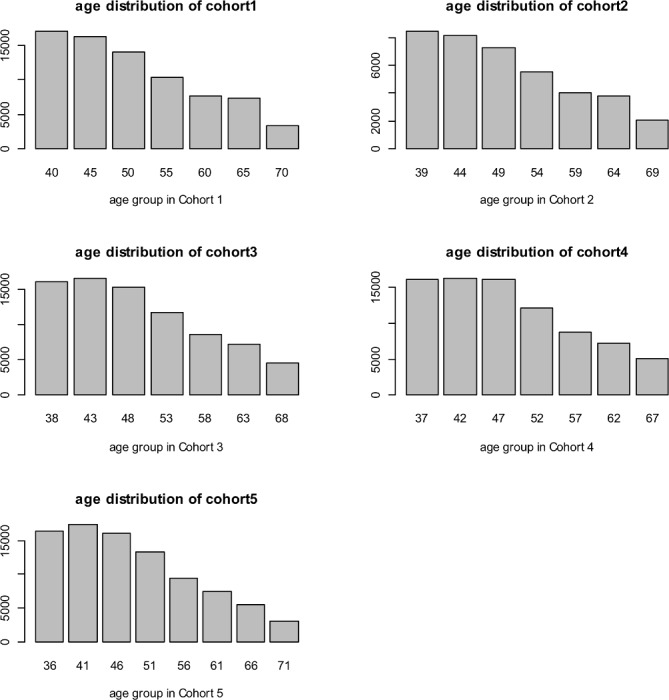
Design: This is a quasi-randomised controlled trial where participants were allocated to five cohorts based on birth year. Four cohorts were invited for an NHS HC between April 2011 and March 2015.
Setting: 151 general practices in Hampshire, England, UK.
Participants: 366 005 participants born 1 April 1940-31 March 1976 eligible for an NHS HC.
Intervention: NHS HC invitation.
Main outcome measures: HC attendance and absolute percentage changes and ORs of (1) detecting cardiovascular disease (CVD) 10-year risk >10% and >20%, smokers, and total cholesterol (TC) >5.5 mmol/L and >7.5 mmol/L; (2) diagnosing hypertension, type 2 diabetes mellitus, chronic kidney disease (CKD) and atrial fibrillation (AF); and (3) new interventions with statins, antihypertensives, antiglycaemics and nicotine replacement therapy (NRT).
Results: HC attendance rose from 12% to 30% between 2011/2012 and 2014/2015 (p<0.001). HC invitation increased detection of CVD risk >10% (2.0%-3.6, p<0.001) and >20% (0.1%-0.6%, p<0.001-0.392), TC >5.5 mmol/L (4.1%-7.0%, p<0.001) and >7.5 mmol/L (0.3%-0.4% p<0.001), hypertension (0.3%-0.6%, p<0.001-0.003), and interventions with statins (0.2%-0.9%, p<0.001-0.017) and antihypertensives (0.1%-0.6%, p<0.001-0.205). There were no consistent differences in detection of smokers, NRT, or diabetes, AF or CKD. Multivariate analyses showed associations between HC invitation and detecting CVD risk >10% (OR 8.01, 95% CI 7.34 to 8.73) and >20% (5.86, 4.83 to 7.10), TC >5.5 mmol/L (3.72, 3.57 to 3.89) and >7.5 mmol/L (2.89, 2.46 to 3.38), and diagnoses of hypertension (1.33, 1.20 to 1.47) and diabetes (1.34, 1.12 to 1.61). OR of CVD risk >10% plus statin and >20% plus statin, respectively, was 2.90 (2.36 to 3.57) and 2.60 (1.92 to 3.52), and for hypertension plus antihypertensive was 1.33 (1.18 to 1.50). There were no associations with AF, CKD, antiglycaemics or NRT. Detection of several risk factors varied inversely by deprivation.
Conclusions: HC invitation increased detection of cardiovascular risk factors, but corresponding increases in evidence-based interventions were modest.
Keywords: cardiovascular risk management; cardiovascular risk screening; health checks; population screening.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for. Lancet 2018;392(10159:1789–858. - PMC - PubMed
-
- Department of Health Economic modelling for vascular checks. London: Department of Health, 2008.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous