

A tailored molecular profiling programme for children with cancer to identify clinically actionable genetic alterations
- PMID: 31543384
- PMCID: PMC6839402
- DOI: 10.1016/j.ejca.2019.07.027
A tailored molecular profiling programme for children with cancer to identify clinically actionable genetic alterations
Abstract
Background: For children with cancer, the clinical integration of precision medicine to enable predictive biomarker-based therapeutic stratification is urgently needed.
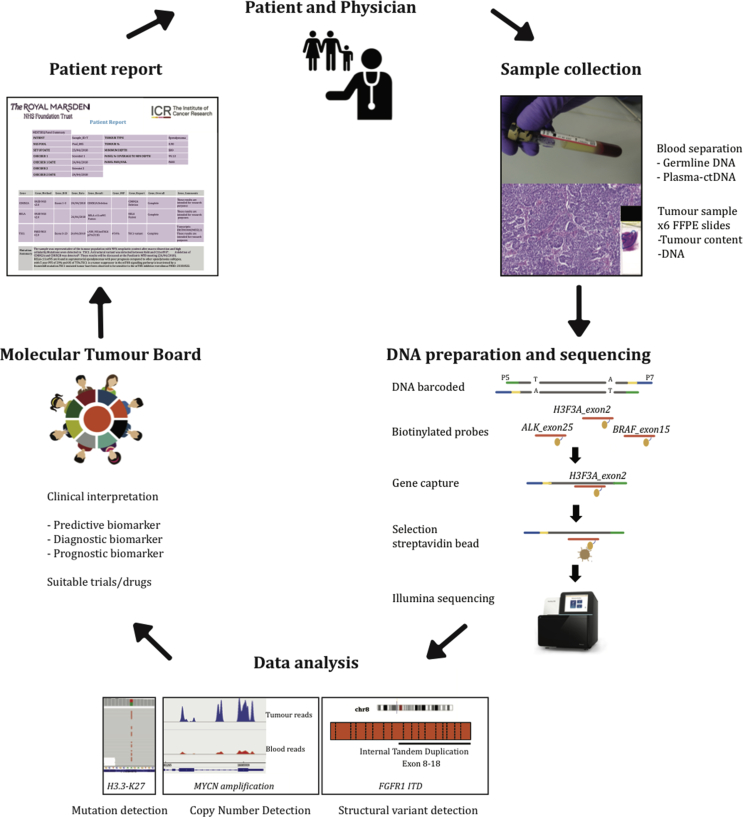
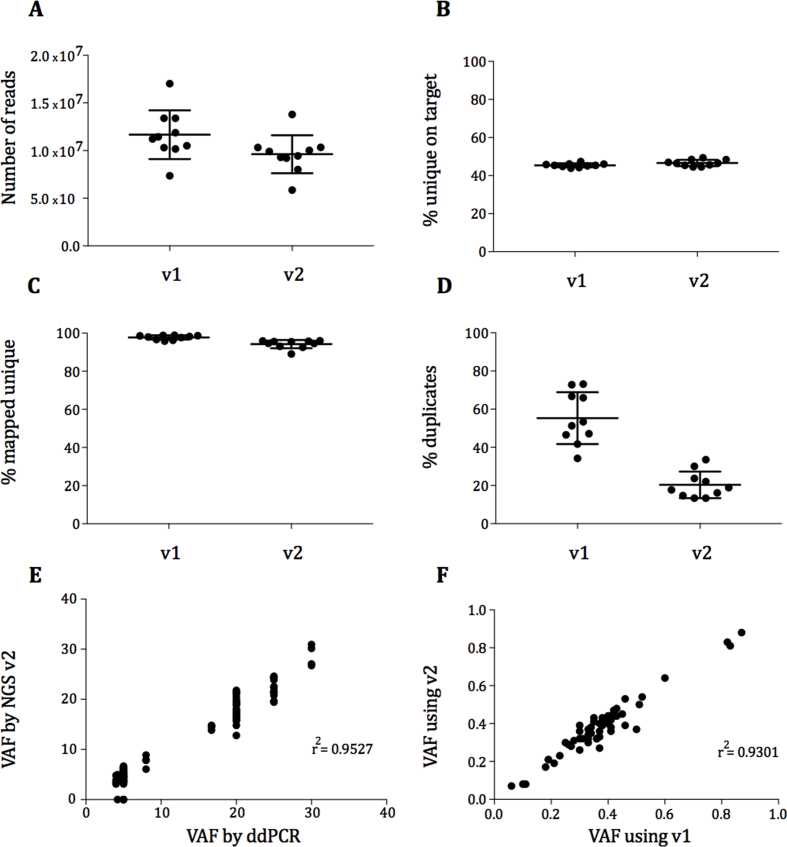
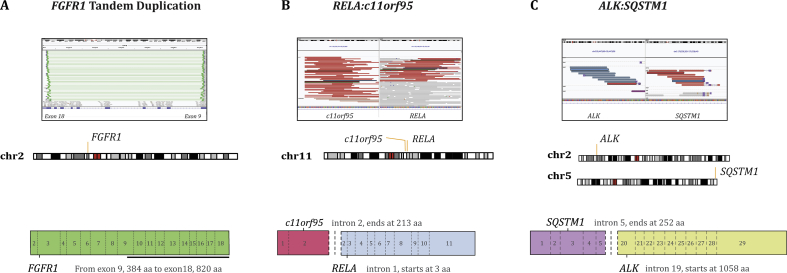
Methods: We have developed a hybrid-capture next-generation sequencing (NGS) panel, specifically designed to detect genetic alterations in paediatric solid tumours, which gives reliable results from as little as 50 ng of DNA extracted from formalin-fixed paraffin-embedded (FFPE) tissue. In this study, we offered an NGS panel, with clinical reporting via a molecular tumour board for children with solid tumours. Furthermore, for a cohort of 12 patients, we used a circulating tumour DNA (ctDNA)-specific panel to sequence ctDNA from matched plasma samples and compared plasma and tumour findings.
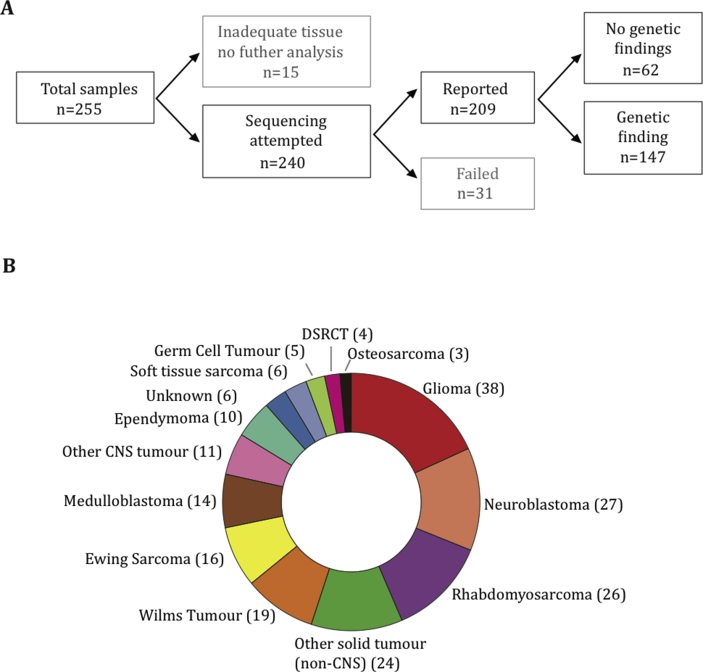
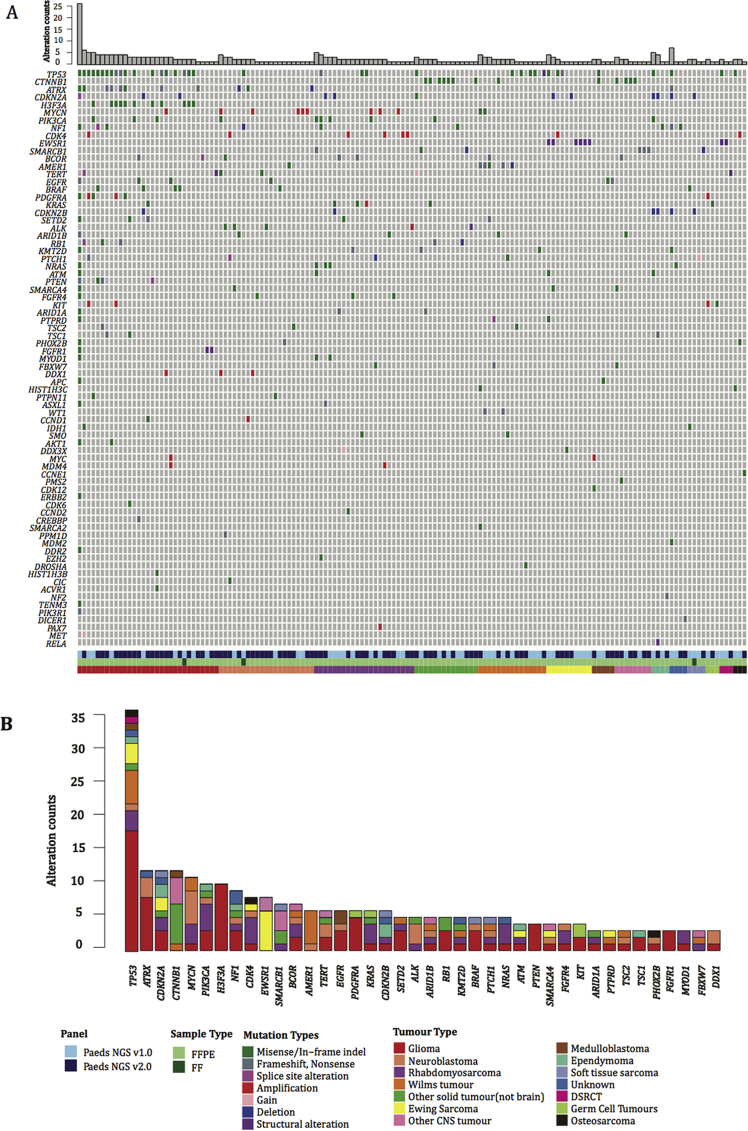
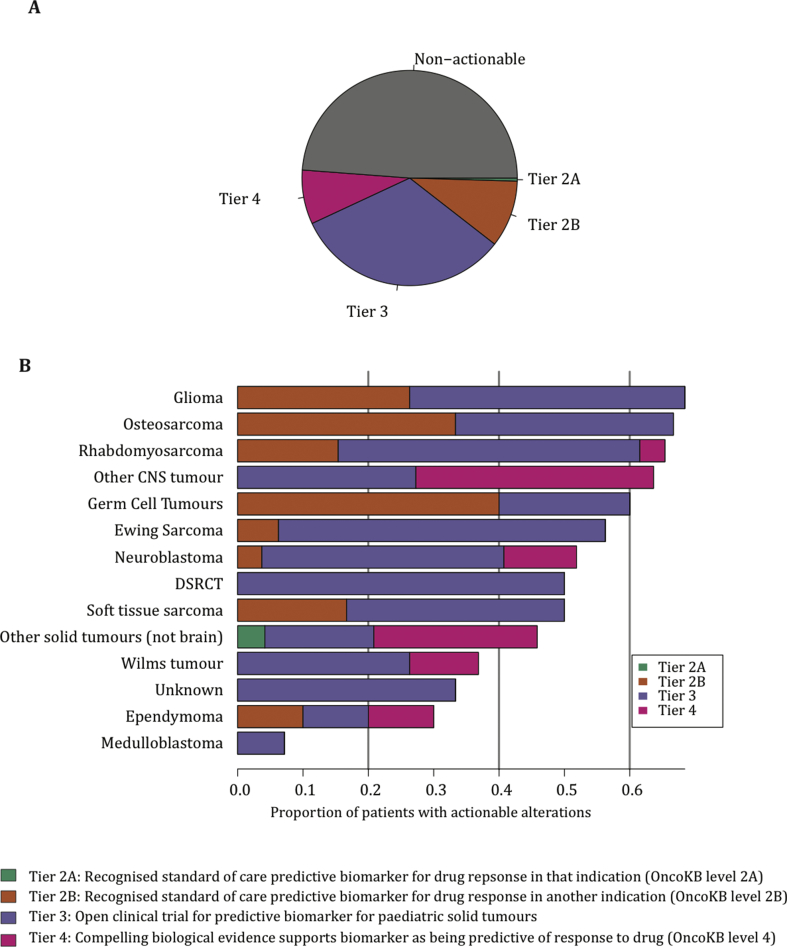
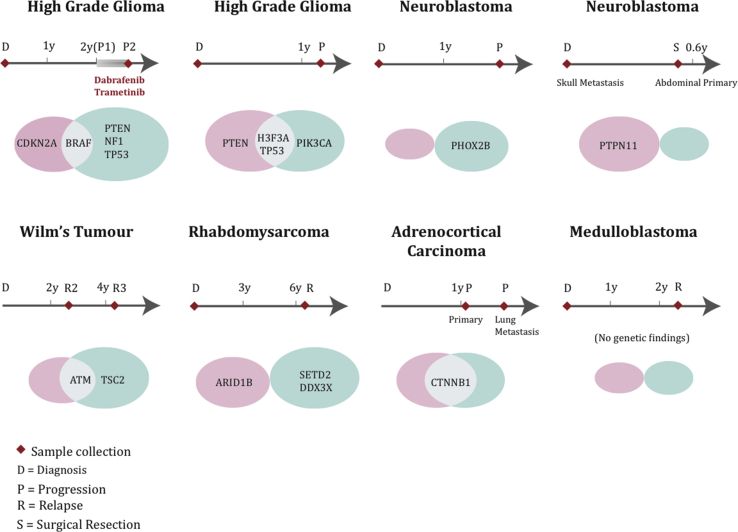
Results: A total of 255 samples were submitted from 223 patients for the NGS panel. Using FFPE tissue, 82% of all submitted samples passed quality control for clinical reporting. At least one genetic alteration was detected in 70% of sequenced samples. The overall detection rate of clinically actionable alterations, defined by modified OncoKB criteria, for all sequenced samples was 51%. A total of 8 patients were sequenced at different stages of treatment. In 6 of these, there were differences in the genetic alterations detected between time points. Sequencing of matched ctDNA in a cohort of extracranial paediatric solid tumours also identified a high detection rate of somatic alterations in plasma.
Conclusion: We demonstrate that tailored clinical molecular profiling of both tumour DNA and plasma-derived ctDNA is feasible for children with solid tumours. Furthermore, we show that a targeted NGS panel-based approach can identify actionable genetic alterations in a high proportion of patients.
Keywords: Circulating tumour DNA; Clinical targeted sequencing; Paediatric oncology; Personalised medicine.
Crown Copyright © 2019. Published by Elsevier Ltd. All rights reserved.
Figures
References
-
- Fiore R.N., Goodman K.W. Precision medicine ethics: selected issues and developments in next-generation sequencing, clinical oncology, and ethics. Curr Opin Oncol. 2016;28(1):83–87. - PubMed
-
- Tuff-Lacey A. A collaborative approach to enabling stratified cancer medicine in the UK. Drug Discov Today. 2015;20(12):1414–1418. - PubMed
-
- Do K., O'Sullivan Coyne G., Chen A.P. An overview of the NCI precision medicine trials-NCI MATCH and MPACT. Chin Clin Oncol. 2015;4(3):31. - PubMed
-
- Kim G. FDA approval summary: olaparib monotherapy in patients with deleterious germline BRCA-mutated advanced ovarian cancer treated with three or more lines of chemotherapy. Clin Cancer Res. 2015;21(19):4257–4261. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
