

Lymphocyte-to-monocyte ratio effectively predicts survival outcome of patients with obstructive colorectal cancer
- PMID: 31543687
- PMCID: PMC6737316
- DOI: 10.3748/wjg.v25.i33.4970
Lymphocyte-to-monocyte ratio effectively predicts survival outcome of patients with obstructive colorectal cancer
Abstract
Background: Obstructive colorectal cancer (OCC) is always accompanied by severe complications, and the optimal strategy for patients with OCC remains undetermined. Different from emergency surgery (ES), self-expandable metal stents (SEMS) as a bridge to surgery (BTS), could increase the likelihood of primary anastomosis. However, the stent failure and related complications might give rise to a high recurrence rate. Few studies have focused on the indications for either method, and the relationship between preoperative inflammation indexes and the prognosis of OCC is still underestimated.
Aim: To explore the indications for ES and BTS in OCCs based on preoperative inflammation indexes.
Methods: One hundred and twenty-eight patients who underwent ES or BTS from 2008 to 2015 were enrolled. Receiver operating characteristic (ROC) curve analysis was used to define the optimal preoperative inflammation index and its cutoff point. Kaplan-Meier analyses and Cox proportional hazards models were applied to assess the association between the preoperative inflammation indexes and the survival outcomes [overall survival (OS) and disease-free survival (DFS)]. Stratification analysis was performed to identify the subgroups that would benefit from ES or BTS.
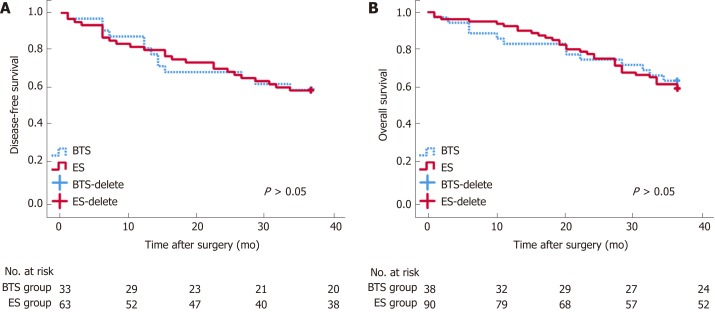
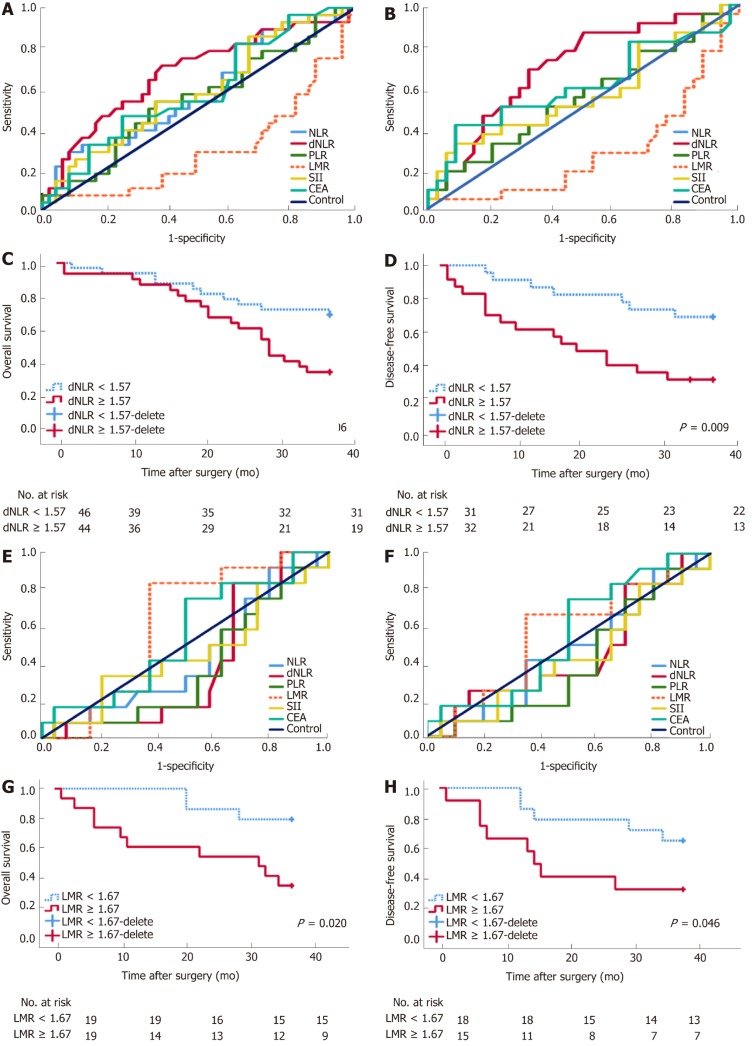
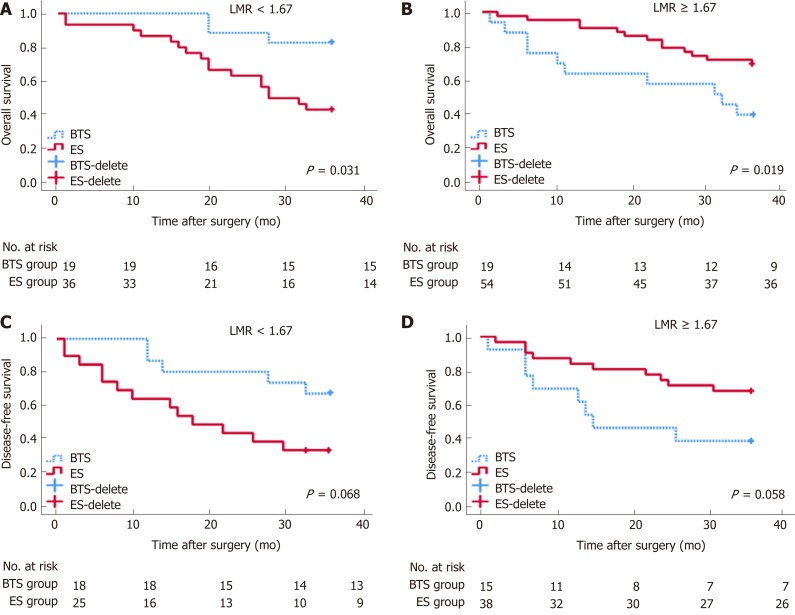
Results: OS and DFS were comparable between the ES and BTS groups (P > 0.05). ROC curve analysis showed derived neutrophil-to-lymphocyte ratio (dNLR) as the optimal biomarker for the prediction of DFS in ES (P < 0.05). Lymphocyte-to-monocyte ratio (LMR) was recommended for BTS with regard to OS and DFS (P < 0.05). dNLR was related to stoma construction (P = 0.001), pneumonia (P = 0.054), and DFS (P = 0.009) in ES. LMR was closely related to lymph node invasion (LVI) (P = 0.009), OS (P = 0.020), and DFS (P = 0.046) in the BTS group. dNLR was an independent risk factor for ES in both OS (P = 0.032) and DFS (P = 0.016). LMR affected OS (P = 0.053) and DFS (P = 0.052) in the BTS group. LMR could differentiate the OS between the ES and BTS groups (P < 0.05).
Conclusion: Preoperative dNLR and LMR could predict OS and DFS in patients undergoing ES and BTS, respectively. For OCC, as the potential benefit group, patients with a low LMR might be preferred for BTS via SEMS insertion.
Keywords: Emergency surgery; Inflammation indexes; Obstructive colorectal cancers; Self-expanding metal stent insertion as a bridge to surgery.
Conflict of interest statement
Conflict-of-interest statement: All authors read and approved the final manuscript and declared no conflicts of interest.
Figures
References
-
- van Hooft JE, van Halsema EE, Vanbiervliet G, Beets-Tan RG, DeWitt JM, Donnellan F, Dumonceau JM, Glynne-Jones RG, Hassan C, Jiménez-Perez J, Meisner S, Muthusamy VR, Parker MC, Regimbeau JM, Sabbagh C, Sagar J, Tanis PJ, Vandervoort J, Webster GJ, Manes G, Barthet MA, Repici A European Society of Gastrointestinal Endoscopy (ESGE) Self-expandable metal stents for obstructing colonic and extracolonic cancer: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Gastrointest Endosc. 2014;80:747–61.e1-75. - PubMed
-
- Yeo HL, Lee SW. Colorectal emergencies: review and controversies in the management of large bowel obstruction. J Gastrointest Surg. 2013;17:2007–2012. - PubMed
-
- Pisano M, Zorcolo L, Merli C, Cimbanassi S, Poiasina E, Ceresoli M, Agresta F, Allievi N, Bellanova G, Coccolini F, Coy C, Fugazzola P, Martinez CA, Montori G, Paolillo C, Penachim TJ, Pereira B, Reis T, Restivo A, Rezende-Neto J, Sartelli M, Valentino M, Abu-Zidan FM, Ashkenazi I, Bala M, Chiara O, De' Angelis N, Deidda S, De Simone B, Di Saverio S, Finotti E, Kenji I, Moore E, Wexner S, Biffl W, Coimbra R, Guttadauro A, Leppäniemi A, Maier R, Magnone S, Mefire AC, Peitzmann A, Sakakushev B, Sugrue M, Viale P, Weber D, Kashuk J, Fraga GP, Kluger I, Catena F, Ansaloni L. 2017 WSES guidelines on colon and rectal cancer emergencies: obstruction and perforation. World J Emerg Surg. 2018;13:36. - PMC - PubMed
-
- Govindarajan A, Naimark D, Coburn NG, Smith AJ, Law CH. Use of colonic stents in emergent malignant left colonic obstruction: a Markov chain Monte Carlo decision analysis. Dis Colon Rectum. 2007;50:1811–1824. - PubMed
-
- Martinez-Santos C, Lobato RF, Fradejas JM, Pinto I, Ortega-Deballón P, Moreno-Azcoita M. Self-expandable stent before elective surgery vs. emergency surgery for the treatment of malignant colorectal obstructions: comparison of primary anastomosis and morbidity rates. Dis Colon Rectum. 2002;45:401–406. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
