

Human Monocyte Subsets and Phenotypes in Major Chronic Inflammatory Diseases
- PMID: 31543877
- PMCID: PMC6728754
- DOI: 10.3389/fimmu.2019.02035
Human Monocyte Subsets and Phenotypes in Major Chronic Inflammatory Diseases
Abstract
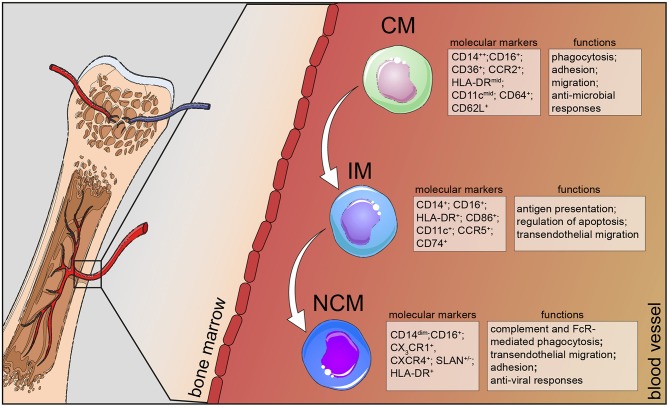
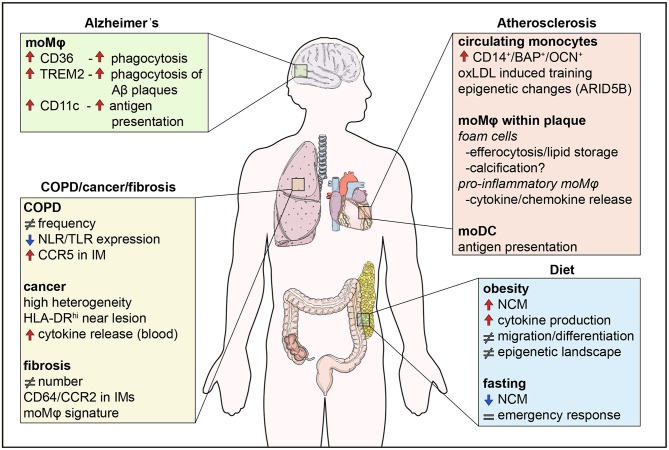
Human monocytes are divided in three major populations; classical (CD14+CD16-), non-classical (CD14dimCD16+), and intermediate (CD14+CD16+). Each of these subsets is distinguished from each other by the expression of distinct surface markers and by their functions in homeostasis and disease. In this review, we discuss the most up-to-date phenotypic classification of human monocytes that has been greatly aided by the application of novel single-cell transcriptomic and mass cytometry technologies. Furthermore, we shed light on the role of these plastic immune cells in already recognized and emerging human chronic diseases, such as obesity, atherosclerosis, chronic obstructive pulmonary disease, lung fibrosis, lung cancer, and Alzheimer's disease. Our aim is to provide an insight into the contribution of human monocytes to the progression of these diseases and highlight their candidacy as potential therapeutic cell targets.
Keywords: atherosclerosis; diet; human monocytes; neurodegeneration; respiratory diseases.
Figures
References
-
- Passlick B, Flieger D, Ziegler-Heitbrock HW. Identification and characterization of a novel monocyte subpopulation in human peripheral blood. Blood. (1989) 74:2527–34. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials