

Treatment decisions in end-stage COPD: who decides how? A cross-sectional survey of different medical specialties
- PMID: 31544110
- PMCID: PMC6745412
- DOI: 10.1183/23120541.00163-2018
Treatment decisions in end-stage COPD: who decides how? A cross-sectional survey of different medical specialties
Abstract
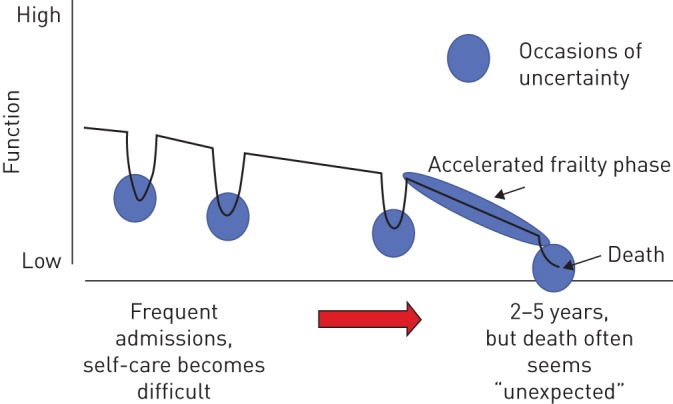
Introduction: End-stage chronic obstructive pulmonary disease (COPD) patients with acute respiratory failure are often treated by representatives from different medical specialties. This study investigates if the choice of treatment is influenced by the medical specialty.
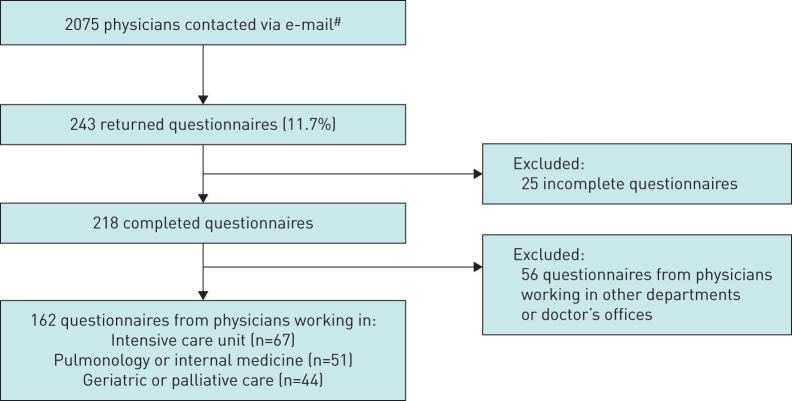
Methods: An online cross-sectional survey among four Austrian medical societies was performed, accompanied by a case vignette of a geriatric end-stage COPD patient with acute respiratory failure. Respondents had to choose between noninvasive ventilation (NIV), a conservative treatment attempt (without NIV) and a palliative approach. Ethical considerations and their impact on decision making were also assessed.
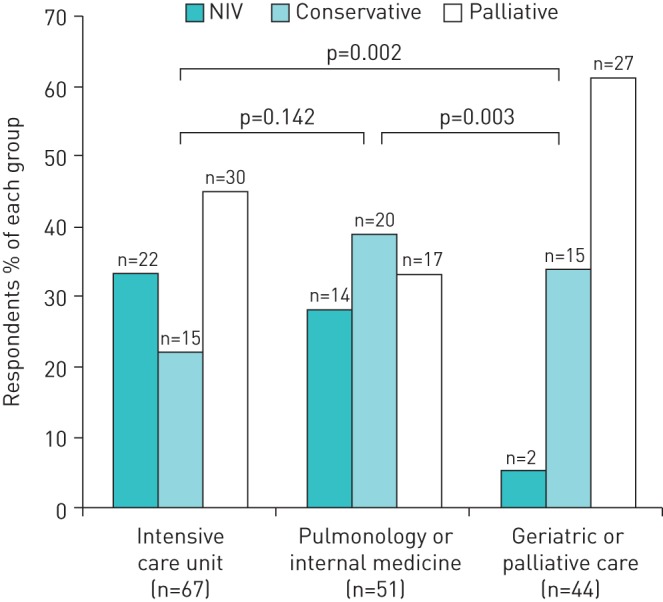
Results: Responses of 162 physicians (67 from intensive care units (ICUs), 51 from pulmonology or internal departments and 44 from geriatric or palliative care) were included. The decision for NIV (instead of a conservative or palliative approach) was associated with working in an ICU (OR 14.9, 95% CI 1.87-118.8) and in a pulmonology or internal department (OR 9.4, 95% CI 1.14-78.42) compared with working in geriatric or palliative care (Model 1). The decision for palliative care was negatively associated with working in a pulmonology or internal department (OR 0.16, 95% CI 0.05-0.47) and (nonsignificantly) in an ICU (OR 0.41, 95% CI 0.15-1.12) (Model 2).
Conclusions: Department association was shown to be an independent predictor for treatment decisions in end-stage COPD with acute respiratory failure. Further research on these differences and influential factors is necessary.
Conflict of interest statement
Conflict of interest: M. Gäbler has nothing to disclose. Conflict of interest: G. Ohrenberger has nothing to disclose. Conflict of interest: G-C. Funk reports a speaker fee from AstraZeneca, service on an advisory board for GSK, a speaker fee from and service on an advisory board for Boehringer Ingelheim, and a speaker fee from Orion Pharma, outside the submitted work.
Figures
Similar articles
-
Noninvasive ventilation for severely acidotic patients in respiratory intermediate care units : Precision medicine in intermediate care units.BMC Pulm Med. 2016 Jul 7;16(1):97. doi: 10.1186/s12890-016-0262-9. BMC Pulm Med. 2016. PMID: 27387544 Free PMC article.
-
Trends in Prevalence and Prognosis in Subjects With Acute Chronic Respiratory Failure Treated With Noninvasive and/or Invasive Ventilation.Respir Care. 2015 Feb;60(2):210-8. doi: 10.4187/respcare.03467. Epub 2014 Nov 18. Respir Care. 2015. PMID: 25406346
-
Early failure of noninvasive ventilation in chronic obstructive pulmonary disease with acute hypercapnic respiratory failure.Intern Emerg Med. 2015 Oct;10(7):855-60. doi: 10.1007/s11739-015-1293-6. Epub 2015 Sep 4. Intern Emerg Med. 2015. PMID: 26341216
-
Noninvasive ventilation as ceiling of therapy in end-stage chronic obstructive pulmonary disease.Chron Respir Dis. 2008;5(3):143-8. doi: 10.1177/1479972308089234. Chron Respir Dis. 2008. PMID: 18684789 Review.
-
[Noninvasive ventilation in palliative care and near the end of life].Rev Mal Respir. 2008 Dec;25(10):1227-36. doi: 10.1016/s0761-8425(08)75088-5. Rev Mal Respir. 2008. PMID: 19107014 Review. French.
Cited by
-
Non-invasive ventilation in the care of patients with chronic obstructive pulmonary disease with palliative care needs: a scoping review.BMC Palliat Care. 2024 Jan 29;23(1):27. doi: 10.1186/s12904-024-01365-y. BMC Palliat Care. 2024. PMID: 38287312 Free PMC article.
-
An Exploratory Study of Physician Decision-Making When Treating Uncontrolled COPD.Int J Chron Obstruct Pulmon Dis. 2024 Jun 18;19:1357-1373. doi: 10.2147/COPD.S454877. eCollection 2024. Int J Chron Obstruct Pulmon Dis. 2024. PMID: 38912054 Free PMC article.
-
Dynamic changes in quality of life in older patients with chronic obstructive pulmonary disease: a 7-year follow up.Health Qual Life Outcomes. 2024 Sep 11;22(1):76. doi: 10.1186/s12955-024-02296-1. Health Qual Life Outcomes. 2024. PMID: 39256723 Free PMC article.
-
Chronic obstructive pulmonary disease trajectory: severe exacerbations and dynamic change in health-related quality of life.BMJ Open Respir Res. 2024 Feb 21;11(1):e002037. doi: 10.1136/bmjresp-2023-002037. BMJ Open Respir Res. 2024. PMID: 38387996 Free PMC article.
-
Multidimensional analysis of anxiety symptoms in patients with chronic obstructive pulmonary disease (COPD).Sci Rep. 2025 Apr 2;15(1):11356. doi: 10.1038/s41598-025-96007-5. Sci Rep. 2025. PMID: 40175594 Free PMC article.
References
-
- Gibson GJ, Loddenkemper R, Lundbäck B, et al. . Respiratory health and disease in Europe: the new European Lung White Book. Eur Respir J 2013; 42: 559–563. - PubMed
-
- Klimathianaki M, Mitrouska I, Georgopoulos D. Management of end-stage chronic obstructive pulmonary disease In: Siafakas NM, ed. Management of Chronic Obstructive Pulmonary Disease (ERS Monograph). Sheffield, European Respiratory Society, 2006; pp. 430–450.
-
- Creagh-Brown B, Shee C. Noninvasive ventilation as ceiling of therapy in end-stage chronic obstructive pulmonary disease. Chron Respir Dis 2008; 5: 143–148. - PubMed
LinkOut - more resources
Full Text Sources