

Discontinuation of Acute Prescription Medication for Migraine: Results From the Chronic Migraine Epidemiology and Outcomes (CaMEO) Study
- PMID: 31544244
- PMCID: PMC6899725
- DOI: 10.1111/head.13642
Discontinuation of Acute Prescription Medication for Migraine: Results From the Chronic Migraine Epidemiology and Outcomes (CaMEO) Study
Abstract
Objective: This analysis assessed migraine-related burden and treatment decisions in Chronic Migraine Epidemiology and Outcomes (CaMEO) Study survey respondents who stopped taking acute prescription medications for migraine.
Background: Migraine is a common yet underdiagnosed and undertreated neurological disease often associated with significant disability. Acute prescription medications are underused, in part because patients discontinue treatment. Rates and reasons for discontinuing acute prescription medications require exploration.
Methods: The CaMEO Study is a longitudinal, Internet-based survey that identified and followed people who met modified ICHD-3 migraine criteria. For this analysis, eligible respondents had used acute prescription medication for migraine in the past but no longer used or kept these treatments on hand (discontinued users). Respondents who reported discontinuing acute prescription treatment answered questions about length of time since last use and reasons for stopping. Reasons for discontinuing were thematically summarized. Monthly headache day frequency, Migraine Disability Assessment (MIDAS), Patient Health Questionnaire 9-item depression screener, Generalized Anxiety Disorder 7-item screener, and the 12-item Allodynia Symptom Checklist were also assessed.
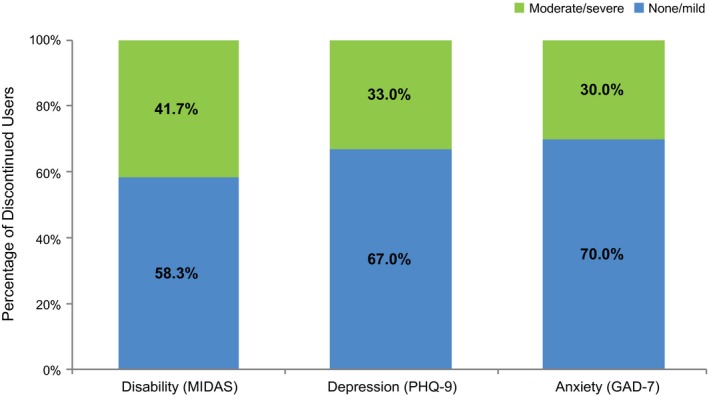
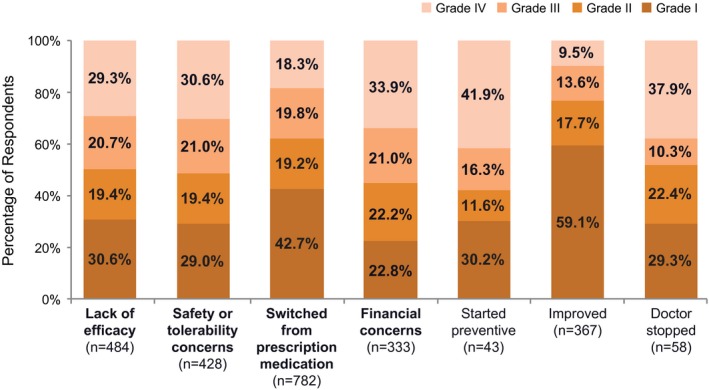
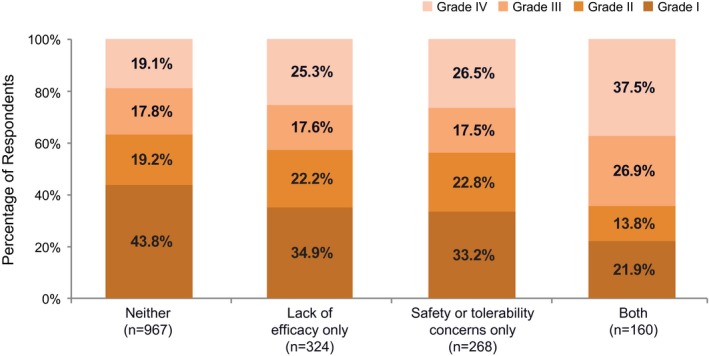
Results: Of 13,624 respondents with migraine, 4840 (35.5%) had ever used acute prescription medications and 1719 (35.5%) of those were discontinued users. Discontinued users had a mean (SD) age of 42.1 (14) years, and 1348/1719 (78.4%) were female. Monthly headache frequency of 0-4 days was reported by 1073/1719 (62.4%) of respondents, 5-9 days by 322/1719 (18.7%), 10-14 days by 135/1719 (7.9%), and ≥15 days by 189/1719 (11.0%). Two-thirds (1160/1719 [67.5%]) of discontinued users reported a receiving migraine (or chronic migraine) diagnosis from a doctor or other health professional in the past. Although all had spoken to a doctor about their headaches, 1504/1719 (87.5%) had stopped having their headaches managed or treated by a doctor for at least 12 months. Only 1 in 5 discontinued users reported being able to work or function normally with a headache, and 717/1719 (41.7%) had moderate to severe disability (MIDAS). Among the most commonly reported reasons for prescription medication discontinuation were switching to non-prescription pain medication (782/1719 [45.5%]), as well as concerns about prescription medication efficacy (484/1719 [28.2%]) and tolerability (428/1719 [24.9%]). Nearly half of respondents who reported either efficacy or tolerability concerns had moderate to severe disability.
Conclusions: People with migraine who discontinue acute prescription medication have a high level of unmet treatment need. The majority cannot work or function normally with headaches, with 646/1719 (37.6%) of discontinued users reporting 5 or more headache days per month.
Keywords: Chronic Migraine Epidemiology and Outcomes; acute treatment; disability; migraine; triptans.
© 2019 The Authors. Headache: The Journal of Head and Face Pain published by Wiley Periodicals, Inc. on behalf of American Headache Society.
Figures
References
-
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators . Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990‐2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390:1211‐1259. - PMC - PubMed
-
- Goadsby PJ, Lipton RB, Ferrari MD. Migraine – Current understanding and treatment. N Engl J Med. 2002;346:257‐270. - PubMed
-
- Silberstein SD. Practice parameter: Evidence‐based guidelines for migraine headache (an evidence‐based review): Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2000;55:754‐762. - PubMed
-
- Bigal ME, Borucho S, Serrano D, Lipton RB. The acute treatment of episodic and chronic migraine in the USA. Cephalalgia. 2009;29:891‐897. - PubMed
-
- Buse DC, Pearlman SH, Reed ML, Serrano D, Ng‐Mak DS, Lipton RB. Opioid use and dependence among persons with migraine: Results of the AMPP study. Headache. 2012;52:18‐36. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
