

Rate and Prognosis of Brain Ischemia in Patients With Lower-Risk Transient or Persistent Minor Neurologic Events
- PMID: 31545347
- PMCID: PMC6763989
- DOI: 10.1001/jamaneurol.2019.3063
Rate and Prognosis of Brain Ischemia in Patients With Lower-Risk Transient or Persistent Minor Neurologic Events
Erratum in
-
Error in Results.JAMA Neurol. 2020 Mar 1;77(3):394. doi: 10.1001/jamaneurol.2019.4873. JAMA Neurol. 2020. PMID: 31930354 Free PMC article. No abstract available.
Abstract
Importance: Early treatment of patients with transient ischemic attack (TIA) reduces the risk of stroke. However, many patients present with symptoms that have an uncertain diagnosis. Patients with motor, speech, or prolonged symptoms are at the highest risk for recurrent stroke and the most likely to undergo comprehensive investigations. Lower-risk patients are much more likely to be cursorily investigated.
Objective: To establish the frequency of acute infarct defined by diffusion restriction detected on diffusion-weighted imaging (DWI) magnetic resonance imaging (MRI) scan (DWI positive).
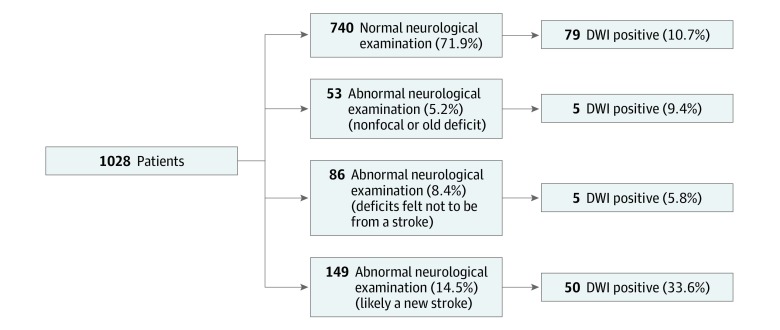
Design, setting, and participants: The Diagnosis of Uncertain-Origin Benign Transient Neurological Symptoms (DOUBT) study was a prospective, observational, international, multicenter cohort study of 1028 patients with low-risk transient or minor symptoms referred to neurology within 8 days of symptom onset. Patients were enrolled between June 1, 2010, and October 31, 2016. Included patients were 40 years or older and had experienced nonmotor or nonspeech minor focal neurologic events of any duration or motor or speech symptoms of short duration (≤5 minutes), with no previous stroke.
Exposures: Patients underwent a detailed neurologic assessment prior to undergoing a brain MRI within 8 days of symptom onset.
Main outcomes and measures: The primary outcome was restricted diffusion on a brain MRI scan (acute stroke).
Results: A total of 1028 patients (522 women and 506 men; mean [SD] age, 63.0 [11.6] years) were enrolled. A total of 139 patients (13.5%) had an acute stroke as defined by diffusion restriction detected on MRI scans (DWI positive). The final diagnosis was revised in 308 patients (30.0%) after undergoing brain MRI. There were 7 (0.7%) recurrent strokes at 1 year. A DWI-positive brain MRI scan was associated with an increased risk of recurrent stroke (relative risk, 6.4; 95% CI, 2.4-16.8) at 1 year. Absence of a DWI-positive lesion on a brain MRI scan had a 99.8% negative predictive value for recurrent stroke. Factors associated with MRI evidence of stroke in multivariable modeling were older age (odds ratio [OR], 1.02; 95% CI, 1.00-1.04), male sex (OR, 2.03; 95% CI, 1.39-2.96), motor or speech symptoms (OR, 2.12; 95% CI, 1.37-3.29), ongoing symptoms at assessment (OR, 1.97; 95% CI, 1.29-3.02), no prior identical symptomatic event (OR, 1.87; 95% CI, 1.12-3.11), and abnormal results of initial neurologic examination (OR, 1.71; 95% CI, 1.11-2.65).
Conclusions and relevance: This study suggested that patients with transient ischemic attack and symptoms traditionally considered low risk carry a substantive risk of acute stroke as defined by diffusion restriction (DWI positive) on a brain MRI scan. Early MRI is required to make a definitive diagnosis.
Conflict of interest statement
Figures
Comment in
-
Benefits of Magnetic Resonance Imaging for Patients Presenting With Low-risk Transient or Persistent Minor Neurologic Deficits.JAMA Neurol. 2019 Dec 1;76(12):1421-1423. doi: 10.1001/jamaneurol.2019.2963. JAMA Neurol. 2019. PMID: 31545348 No abstract available.
-
TIA-Symptome: Oft ist es doch ein Hirnschlag.MMW Fortschr Med. 2020 Mar;162(4):36. doi: 10.1007/s15006-020-0212-6. MMW Fortschr Med. 2020. PMID: 32124351 Review. German. No abstract available.
-
Magnetic Resonance Imaging for Acute Minor Neurological Symptoms: Good for Ruling Stroke in, Not Out.JAMA Neurol. 2020 Jun 1;77(6):775-776. doi: 10.1001/jamaneurol.2020.0661. JAMA Neurol. 2020. PMID: 32310256 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
