

Romiplostim Treatment of Chemotherapy-Induced Thrombocytopenia
- PMID: 31545663
- PMCID: PMC6823892
- DOI: 10.1200/JCO.18.01931
Romiplostim Treatment of Chemotherapy-Induced Thrombocytopenia
Abstract
Purpose: Chemotherapy-induced thrombocytopenia (CIT) leads to delay or reduction in cancer treatment. There is no approved treatment.
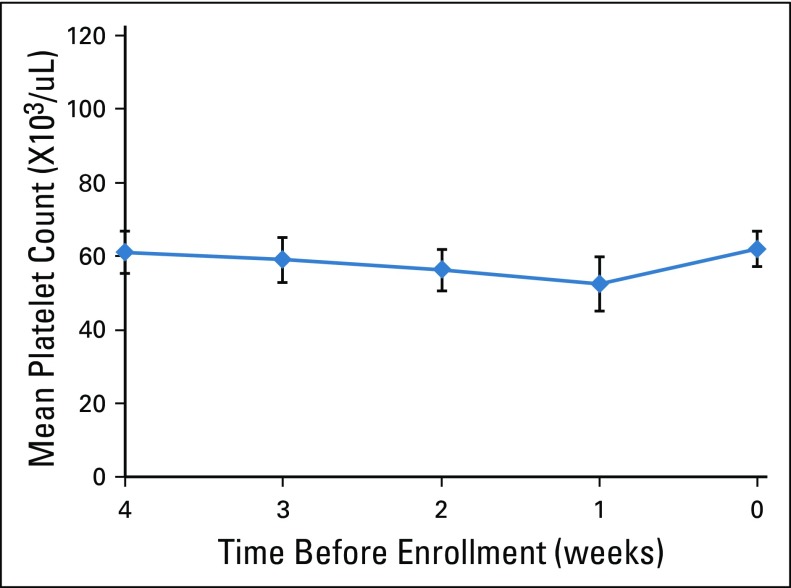
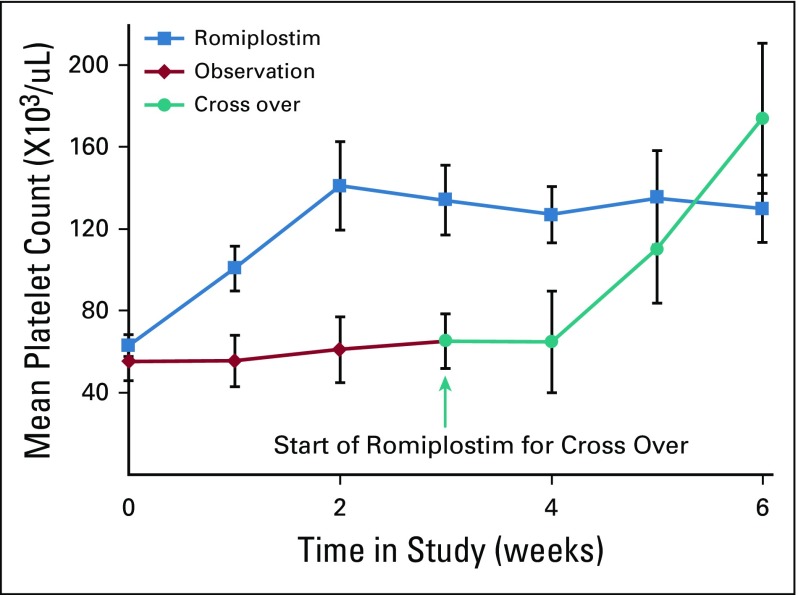
Methods: We conducted a phase II randomized trial of romiplostim versus untreated observation in patients with solid tumors with CIT. Before enrollment, patients had platelets less than 100,000/μL for at least 4 weeks, despite delay or dose reduction of chemotherapy. Patients received weekly titrated romiplostim with a target platelet count of 100,000/μL or more, or were monitored with usual care. The primary end point was correction of platelet count within 3 weeks. Twenty-three patients were treated in a randomization phase, and an additional 37 patients were treated in a single-arm, romiplostim phase. Resumption of chemotherapy without recurrent CIT was a secondary end point.
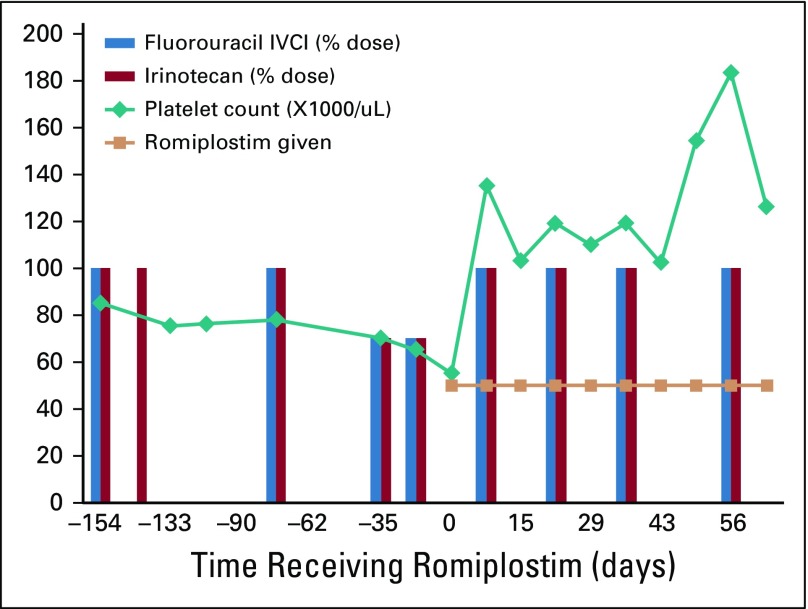
Results: The mean platelet count at enrollment was 62,000/μL. In the randomization phase, 14 of 15 romiplostim-treated patients (93%) experienced correction of their platelet count within 3 weeks, compared with one of eight control patients (12.5%; P < .001). Including all romiplostim-treated patients (N = 52), the mean platelet count at 2 weeks of treatment was 141,000/μL. The mean platelet count in the eight observation patients at 3 weeks was 57,000/μL. Forty-four patients who achieved platelet correction with romiplostim resumed chemotherapy with weekly romiplostim. Only three patients (6.8%) experienced recurrent reduction or delay of chemotherapy because of isolated CIT.
Conclusion: This prospective trial evaluated treatment of CIT with romiplostim. Romiplostim is effective in correcting CIT, and maintenance allows for resumption of chemotherapy without recurrence of CIT in most patients.
Trial registration: ClinicalTrials.gov NCT02052882.
Figures
References
-
- Denduluri N, Patt DA, Wang Y, et al. Dose delays, dose reductions, and relative dose intensity in patients with cancer who received adjuvant or neoadjuvant chemotherapy in community oncology practices. J Natl Compr Canc Netw. 2015;13:1383–1393. - PubMed
-
- Wu Y, Aravind S, Ranganathan G, et al. Anemia and thrombocytopenia in patients undergoing chemotherapy for solid tumors: A descriptive study of a large outpatient oncology practice database, 2000-2007. Clin Ther. 2009;31:2416–2432. - PubMed
-
- Ten Berg MJ, van den Bemt PM, Shantakumar S, et al. Thrombocytopenia in adult cancer patients receiving cytotoxic chemotherapy: Results from a retrospective hospital-based cohort study. Drug Saf. 2011;34:1151–1160. - PubMed
-
- Elting LS, Rubenstein EB, Martin CG, et al. Incidence, cost, and outcomes of bleeding and chemotherapy dose modification among solid tumor patients with chemotherapy-induced thrombocytopenia. J Clin Oncol. 2001;19:1137–1146. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
