

doi: 10.1016/j.healun.2019.08.004.
Epub 2019 Aug 10.
The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Thirty-sixth adult heart transplantation report - 2019; focus theme: Donor and recipient size match
Affiliations
- PMID: 31548031
- PMCID: PMC6816343
- DOI: 10.1016/j.healun.2019.08.004
Item in Clipboard
The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Thirty-sixth adult heart transplantation report - 2019; focus theme: Donor and recipient size match
J Heart Lung Transplant.
2019 Oct.
Erratum in
-
ERRATUM.J Heart Lung Transplant. 2020 Jan;39(1):91. doi: 10.1016/j.healun.2019.11.001. J Heart Lung Transplant. 2020. PMID: 31896417 No abstract available.
No abstract available
Keywords: heart transplant; immunosuppression; organ donation; rejection; survival.
Conflict of interest statement
Disclosure statement
K.K.K. serves as a scientific advisor and speaker for CareDx, Inc; L.P. serves as a speaker for Thermofisher, Sandoz, One Lambda and Novartis, and is an advisory board member for Qiagen and Novartis; J.S. serves as a consultant for Medtronic and Abbott; J.R. serves as a consultant for Bayer, Novartis, Amgen, and CSL Behring, and A.Z. serves on the speakers bureau of Paragonix, Novartis, Mallincrodt, Sanofi-Genzyme, Franz K€ohler Chemie and on the advisory board for Chiesi. M.H., D.H., T.S., B.M., W.C., A.R. and A.S. have no conflicts to disclose.
Figures
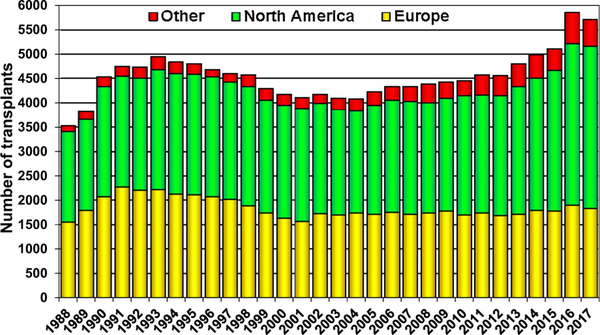
Number of heart transplants (adult and pediatric) by year (transplants: 1988–2017) and geographic region.
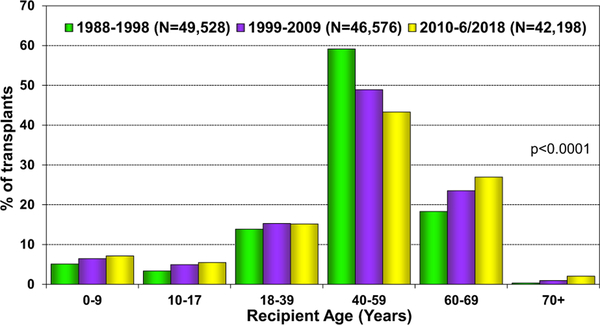
Recipient age distribution (adult and pediatric) by era.
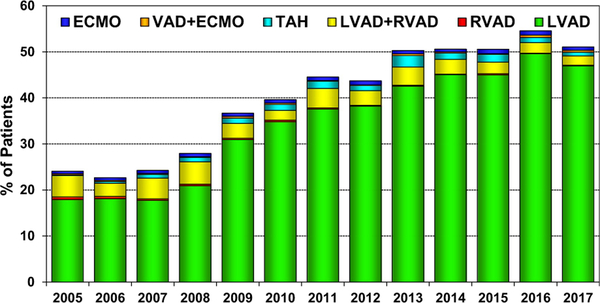
Percent of patients bridged with mechanical circulatory support by year and device type (adult heart transplants: 2005–2017); ECMO: extracorporeal membrane oxygenation; LVAD: left ventricular assist device; RVAD: right ventricular assist device; TAH: total artificial heart; VAD: ventricular assist device.
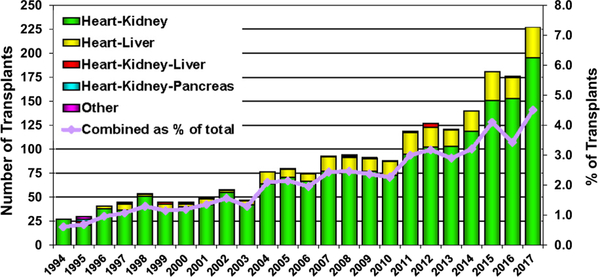
Number and percent of multiorgan transplants reported by year and type of transplant (adult heart transplants; 1994–2017).
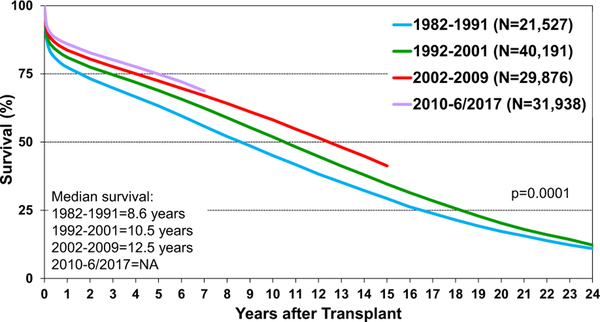
Kaplan-Meier survival by era (adult heart transplants: January 1982–June 2017). NA, not available.
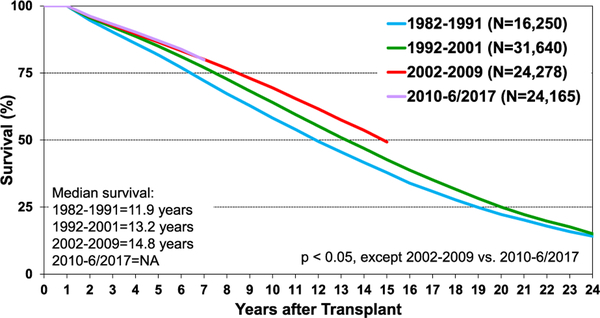
Kaplan-Meier survival by era, conditional on survival to 1 year after transplant (adult heart transplants: January 1982–June 2017). NA, not available.
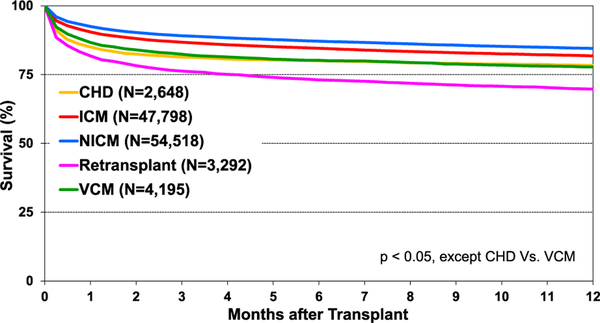
Kaplan-Meier survival within 1 year of transplant by diagnosis (adult heart transplants: January 1985–June 2017); CHD: congenital heart disease; ICM: ischemic cardiomyopathy; NICM: non-ischemic cardiomyopathy; VCM: valvular cardiomyopathy.
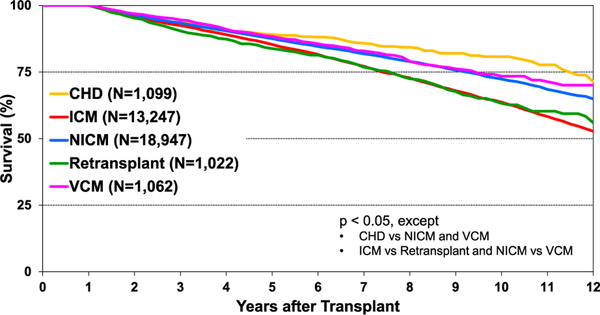
Kaplan-Meier survival by diagnosis, conditional on survival to 1 year after transplant (adult heart transplants: January 2005–June 2017); CHD: congenital heart disease; ICM: ischemic cardiomyopathy; NICM: non-ischemic cardiomyopathy; VCM: valvular cardiomyopathy.
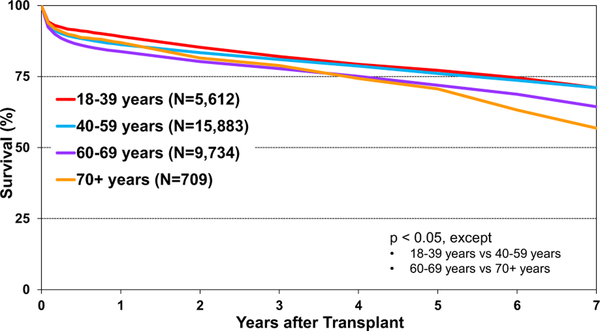
Kaplan-Meier survival by recipient age group (years) (adult heart transplants: January 2010–June 2017).
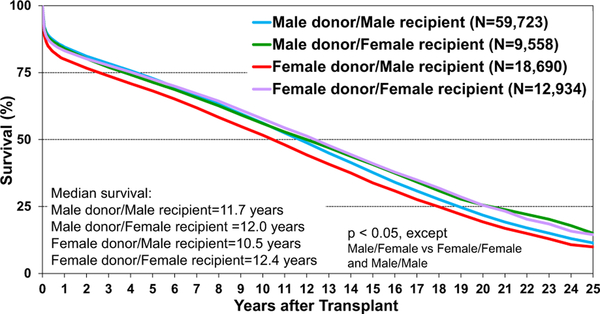
Kaplan-Meier survival by donor/recipient sex (adult heart transplants: January 1992–June 2017).
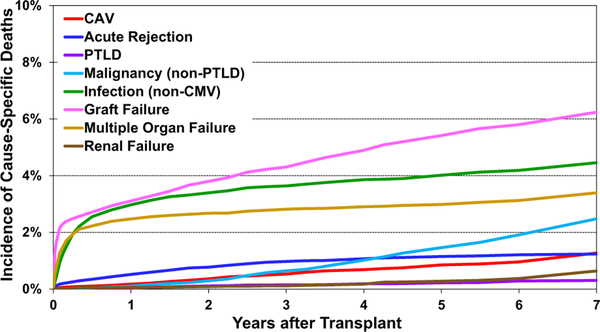
Cumulative incidence of leading causes of death (adult heart transplants: January 2010–June 2017); CAV: cardiac allograft vasculopathy; CMV: cytomegalovirus; PTLD: posttransplant lymphoproliferative disorder.
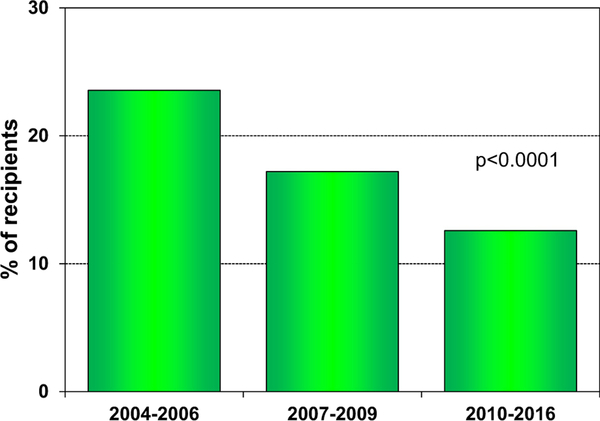
Percent of recipients experiencing treated rejection between transplant discharge and 1-year follow-up, by transplant era (adult heart transplants: 2004–2016).
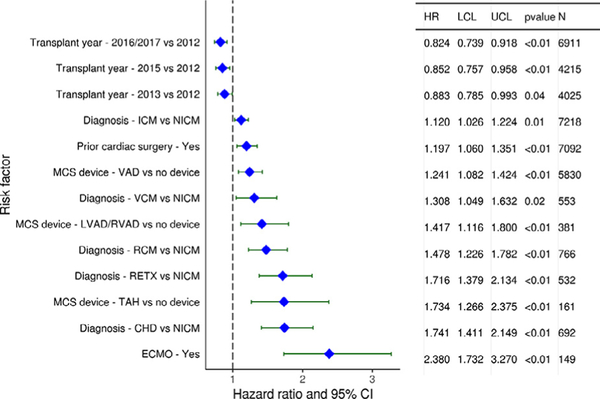
Categorical risk factors for 1-year mortality (adult heart transplants: 2012−June 2017). CHD: congenital heart disease; ECMO: extracorporeal membrane oxygenation; HR, hazard ratio; ICM: ischemic cardiomyopathy; LCL, lower confidence limit; LVAD: left ventricular assist device; MCS: mechanical circulatory support; NICM: non-ischemic cardiomyopathy; RCM: restrictive cardiomyopathy; RETX: retransplant; RVAD: right ventricular assist device; TAH: total artificial heart; UCL, upper confidence limit; VAD: ventricular assist device; VCM: valvular cardiomyopathy.
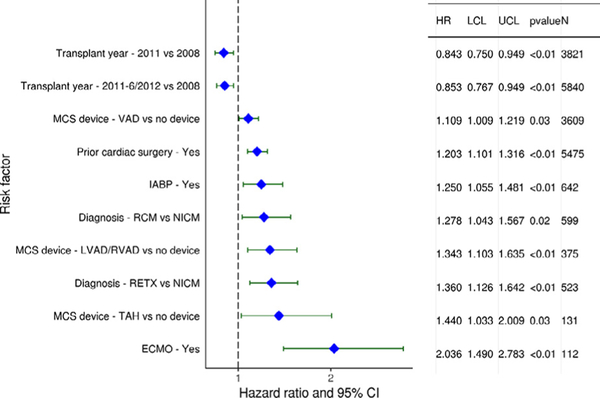
Statistically significant categorical risk factors for 5-year mortality (adult heart transplants: 2008–June 2013). CI, confidence interval; ECMO: extracorporeal membrane oxygenation; HR, hazard ratio; IABP: intra-aortic balloon pump; LCL, lower confidence limit; LVAD: left ventricular assist device; MCS: mechanical circulatory support; NICM: non-ischemic cardiomyopathy; RCM: restrictive cardiomyopathy; RETX: retransplant; RVAD: right ventricular assist device; TAH: total artificial heart; UCL, upper confidence limit; VAD: ventricular assist device.
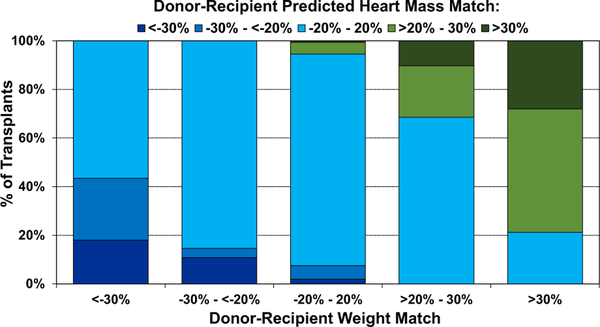
Distribution of donor-recipient predicted heart mass (PHM) match by donor-recipient weight match (adult heart transplant: January 2010–June 2018).
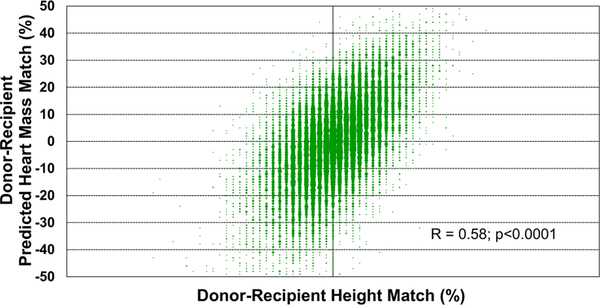
Donor-recipient predicted heart mass match by donor-recipient height match (adult heart transplant: January 2010–June 2018).
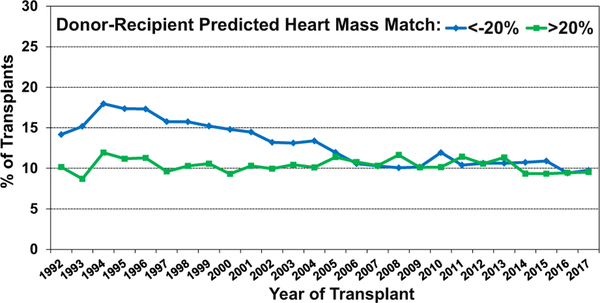
Transplants with donor-recipient predicted heart mass match of <−20% and >20% by transplant year (adult heart transplants: January 1992–December 2017).
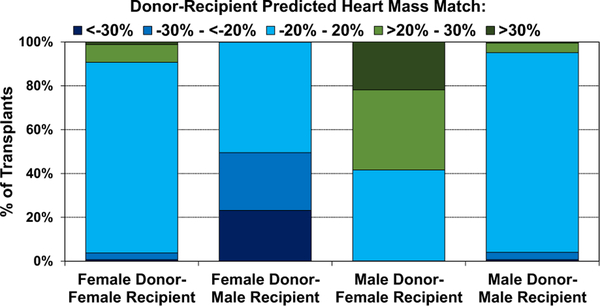
Distribution of donor-recipient predicted heart mass match by donor-recipient sex combinations (adult heart transplants: January 2010–June 2018).
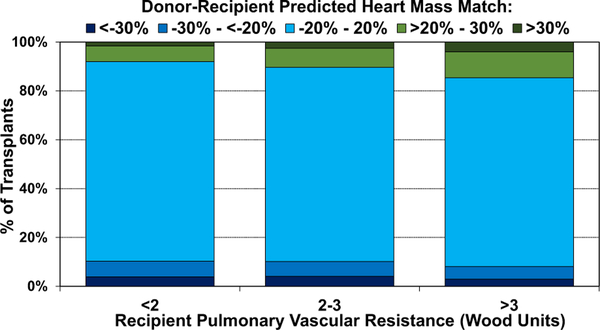
Distribution of donor-recipient predicted heart mass match by recipient pulmonary vascular resistance (adult heart transplants: January 2010–June 2018).
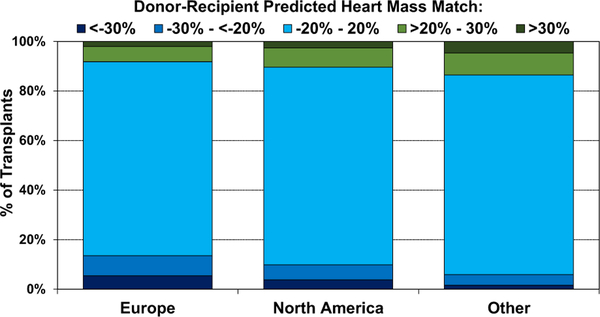
Distribution of donor-recipient predicted heart mass match by geographic location (adult heart transplants: January 2010–June 2018).
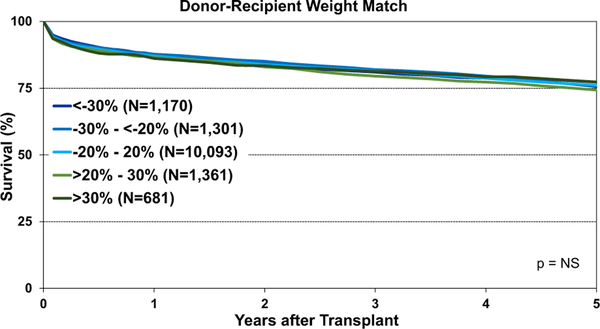
Kaplan-Meier survival by donor-recipient weight match (adult heart transplants: January 2008–June 2013). NS, not significant.
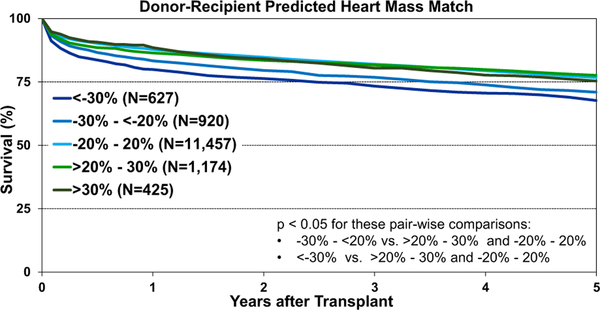
Kaplan-Meier survival by donor-recipient predicted heart mass match (adult heart transplants: January 2008–June 2013).
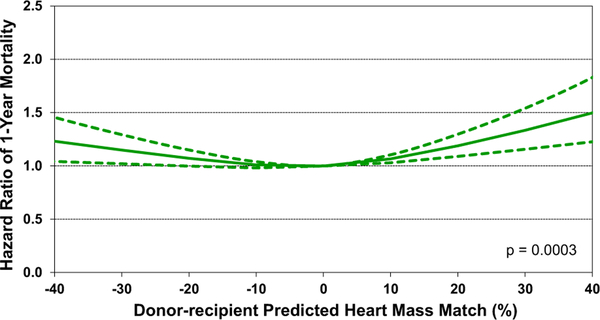
Multivariable hazard ratio plot for 1-year mortality by donor-recipient predicted heart mass match compared to no mismatch (adult heart transplants: 2012–June 2017).
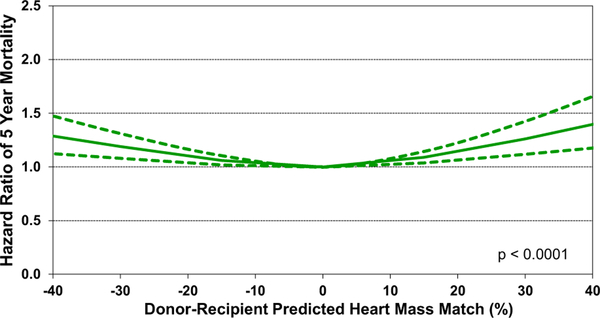
Multivariable hazard ratio plot for 5-year mortality, by donor-recipient predicted heart mass match, compared to no mismatch (adult heart transplants: 2008–June 2013).
References
-
- Blackbourne LH, Tribble CG, Langenburg SE, et al. Successful use of undersized donors for orthotopic heart transplantation—with a caveat. Ann Thorac Surg 1994;57:1472–6. - PubMed
-
- Sethi GK, Lanauze P, Rosado LJ, et al. Clinical significance of weight difference between donor and recipient in heart transplantation. J Thorac Cardiovasc Surg 1993;106:444–8. - PubMed
-
- Taghavi S, Wilson LM, Brann SH, Gaughan J, Mangi AA. Cardiac transplantation can be safely performed with low donor-to-recipient body weight ratios. J Card Fail 2012;18:688–93. - PubMed
-
- Kransdorf EP, Kittleson MM, Benck LR, et al. Predicted heart mass is the optimal metric for size match in heart transplantation. J Heart Lung Transplant 2019;38:156–65. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
