

How to increase the resectability of initially unresectable colorectal liver metastases: A surgical perspective
- PMID: 31549007
- PMCID: PMC6749948
- DOI: 10.1002/ags3.12276
How to increase the resectability of initially unresectable colorectal liver metastases: A surgical perspective
Abstract
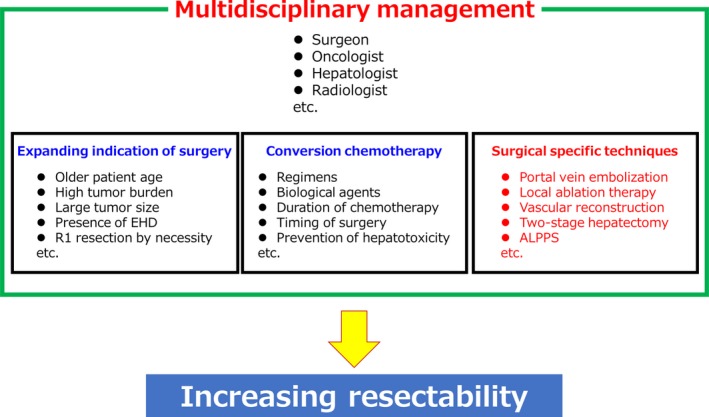
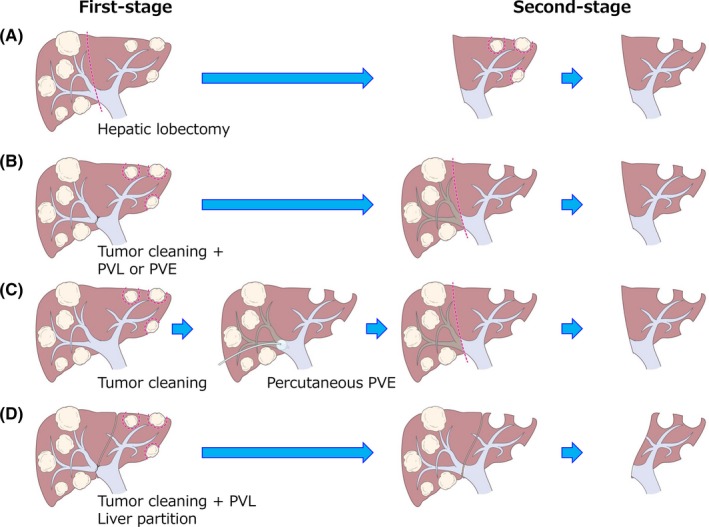
Although surgical resection is the only treatment of choice that can offer prolonged survival and a chance of cure in patients with colorectal liver metastases (CRLM), nearly 80% of patients are deemed to be unresectable at the time of diagnosis. Considerable efforts have been made to overcome this initial unresectability, including expanding the indication of surgery, the advent of conversion chemotherapy, and development and modification of specific surgical techniques, regulated under multidisciplinary approaches. In terms of specific surgical techniques, portal vein ligation/embolization can increase the volume of future liver remnant and thereby reduce the risk of hepatic insufficiency and death after major hepatectomy. For multiple bilobar CRLM that were traditionally considered unresectable even with preoperative chemotherapy and portal vein embolization, two-stage hepatectomy was introduced and has been adopted worldwide with acceptable short- and long-term outcomes. Recently, ALPPS (associating liver partition and portal vein ligation for staged hepatectomy) was reported as a novel variant of two-stage hepatectomy. Although issues regarding safety remain unresolved, rapid future liver remnant hypertrophy and subsequent shorter intervals between the two stages lead to a higher feasibility rate, reaching 98%. In addition, adding radiofrequency ablation and vascular resection and reconstruction techniques can allow expansion of the pool of patients with CRLM who are candidates for liver resection and thus a cure. In this review, we discuss specific techniques that may expand the criteria for resectability in patients with initially unresectable CRLM.
Keywords: ALPPS; colorectal liver metastases; conversion surgery; two‐stage hepatectomy.
Figures
References
-
- Geoghegan JG, Scheele J. Treatment of colorectal liver metastases. Br J Surg. 1999;86(2):158–69. - PubMed
-
- Leonard GD, Brenner B, Kemeny NE. Neoadjuvant chemotherapy before liver resection for patients with unresectable liver metastases from colorectal carcinoma. J Clin Oncol. 2005;23(9):2038–48. - PubMed
-
- Leporrier J, Maurel J, Chiche L, Bara S, Segol P, Launoy G. A population‐based study of the incidence, management and prognosis of hepatic metastases from colorectal cancer. Br J Surg. 2006;93(4):465–74. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
