

Association of obesity with heart failure outcomes in 11 Asian regions: A cohort study
- PMID: 31550265
- PMCID: PMC6759142
- DOI: 10.1371/journal.pmed.1002916
Association of obesity with heart failure outcomes in 11 Asian regions: A cohort study
Abstract
Background: Asians are predisposed to a lean heart failure (HF) phenotype. Data on the 'obesity paradox', reported in Western populations, are scarce in Asia and have only utilised the traditional classification of body mass index (BMI). We aimed to investigate the association between obesity (defined by BMI and abdominal measures) and HF outcomes in Asia.
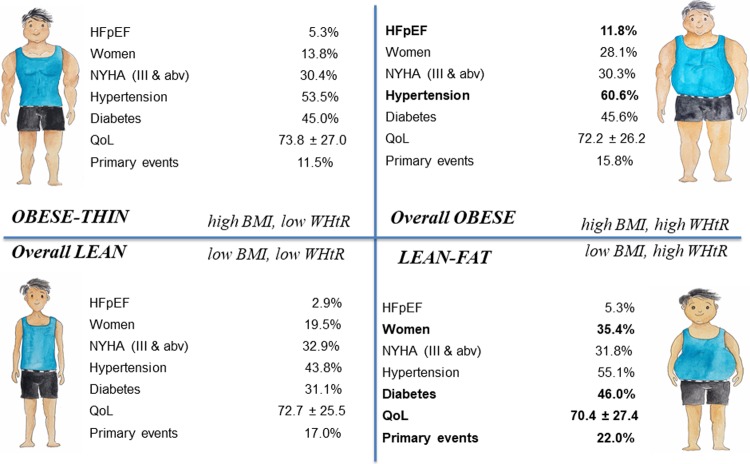
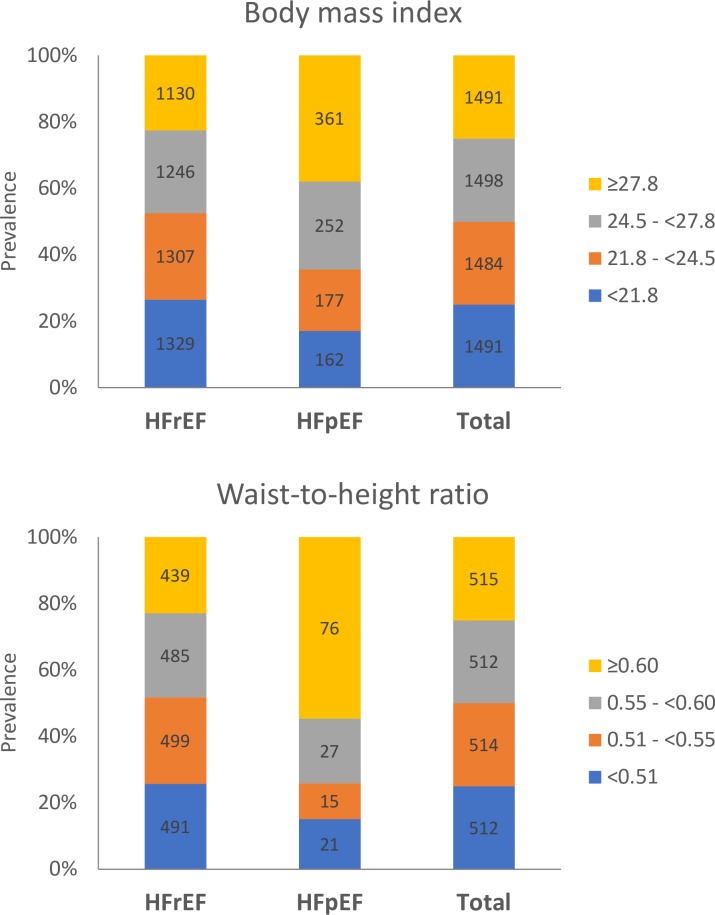
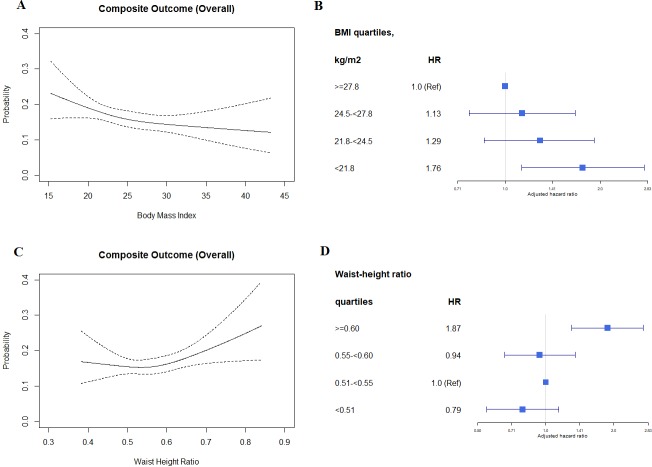
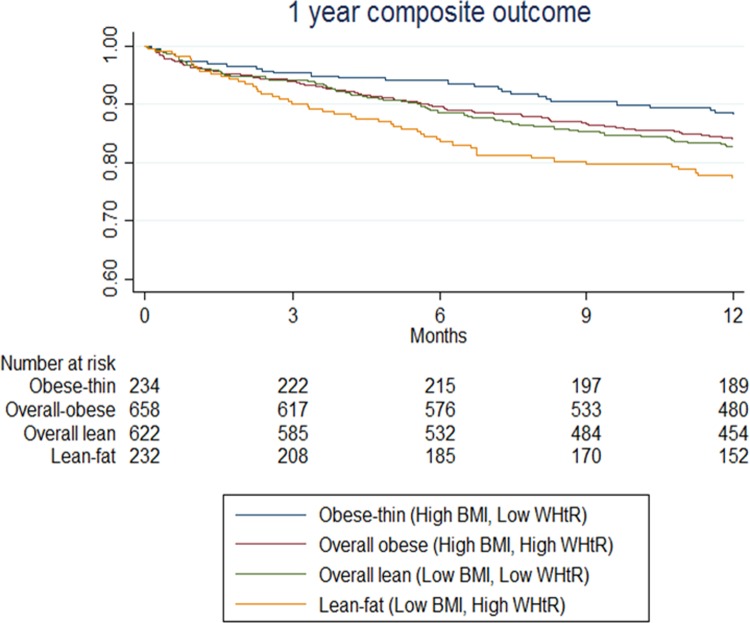
Methods and findings: Utilising the Asian Sudden Cardiac Death in Heart Failure (ASIAN-HF) registry (11 Asian regions including Taiwan, Hong Kong, China, India, Malaysia, Thailand, Singapore, Indonesia, Philippines, Japan, and Korea; 46 centres with enrolment between 1 October 2012 and 6 October 2016), we prospectively examined 5,964 patients with symptomatic HF (mean age 61.3 ± 13.3 years, 26% women, mean BMI 25.3 ± 5.3 kg/m2, 16% with HF with preserved ejection fraction [HFpEF; ejection fraction ≥ 50%]), among whom 2,051 also had waist-to-height ratio (WHtR) measurements (mean age 60.8 ± 12.9 years, 24% women, mean BMI 25.0 ± 5.2 kg/m2, 7% HFpEF). Patients were categorised by BMI quartiles or WHtR quartiles or 4 combined groups of BMI (low, <24.5 kg/m2 [lean], or high, ≥24.5 kg/m2 [obese]) and WHtR (low, <0.55 [thin], or high, ≥0.55 [fat]). Cox proportional hazards models were used to examine a 1-year composite outcome (HF hospitalisation or mortality). Across BMI quartiles, higher BMI was associated with lower risk of the composite outcome (ptrend < 0.001). Contrastingly, higher WHtR was associated with higher risk of the composite outcome. Individuals in the lean-fat group, with low BMI and high WHtR (13.9%), were more likely to be women (35.4%) and to be from low-income countries (47.7%) (predominantly in South/Southeast Asia), and had higher prevalence of diabetes (46%), worse quality of life scores (63.3 ± 24.2), and a higher rate of the composite outcome (51/232; 22%), compared to the other groups (p < 0.05 for all). Following multivariable adjustment, the lean-fat group had higher adjusted risk of the composite outcome (hazard ratio 1.93, 95% CI 1.17-3.18, p = 0.01), compared to the obese-thin group, with high BMI and low WHtR. Results were consistent across both HF subtypes (HFpEF and HF with reduced ejection fraction [HFrEF]; pinteraction = 0.355). Selection bias and residual confounding are potential limitations of such multinational observational registries.
Conclusions: In this cohort of Asian patients with HF, the 'obesity paradox' is observed only when defined using BMI, with WHtR showing the opposite association with the composite outcome. Lean-fat patients, with high WHtR and low BMI, have the worst outcomes. A direct correlation between high WHtR and the composite outcome is apparent in both HFpEF and HFrEF.
Trial registration: Asian Sudden Cardiac Death in HF (ASIAN-HF) Registry ClinicalTrials.gov Identifier: NCT01633398.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: CSPL served as a guest editor on PLOS Medicine's Cardiovascular Disease Special Issue. Unrelated to present work, CSPL is supported by a Clinician Scientist Award from the National Medical Research Council Singapore, non-financial support from Boston Scientific, non-financial support from Bayer, non-financial support from Thermofisher, non-financial support from Vifor Pharma, other from Bayer, other from Novartis, other from Takeda, other from Merck, other from Astra Zeneca, other from Janssen Research & Development, other from LLC, other from Menarini, other from Boehringer Ingelheim, other from Abbott Diagnostics, from DC Devices, outside the submitted work; In addition, CSPL has a patent PCT/SG2016/050217 pending. AMR is supported by a Singapore Translational Research (STaR) award from the National Medical Research Council Singapore, is a named investigator on projects supported by grants from Boston Scientific, Bayer, Astra Zeneca, Roche Diagnostics and has received research support in kind Thermo Fisher, Roche Diagnostics and Abbott Laboratories and other from Novartis. All other authors report no conflict of interest, financial or otherwise.
Figures
References
-
- World Health Organization. Obesity and overweight. Geneva: World Health Organization; 2018. [cited 2019 Aug 27]. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
-
- Lam CS, Teng T-HK, Tay WT, Anand I, Zhang S, Shimizu W, et al. Regional and ethnic differences among patients with heart failure in Asia: the Asian sudden cardiac death in heart failure registry. Eur Heart J. 2016;37(41):3141–53. - PubMed
-
- WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9403):157–63. - PubMed
-
- Haass M, Kitzman DW, Anand IS, Miller A, Zile MR, Massie BM, et al. Body mass index and adverse cardiovascular outcomes in heart failure patients with preserved ejection fraction: results from the Irbesartan in Heart Failure with Preserved Ejection Fraction (I-PRESERVE) trial. Circ Heart Fail. 2011;4(3):324–31. 10.1161/CIRCHEARTFAILURE.110.959890 - DOI - PMC - PubMed
-
- Kenchaiah S, Pocock SJ, Wang D, Finn PV, Zornoff LA, Skali H, et al. Body mass index and prognosis in patients with chronic heart failure: insights from the Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity (CHARM) program. Circulation. 2007;116(6):627–36. 10.1161/circulationaha.106.679779 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
