

Risk of myocardial infarction among people living with HIV: an updated systematic review and meta-analysis
- PMID: 31551371
- PMCID: PMC6773316
- DOI: 10.1136/bmjopen-2018-025874
Risk of myocardial infarction among people living with HIV: an updated systematic review and meta-analysis
Abstract
Objective: Cardiovascular disease (CVD) is one of the leading non-AIDS-defining causes of death among HIV-positive (HIV+) individuals. However, the evidence surrounding specific components of CVD risk remains inconclusive. We conducted a systematic review and meta-analysis to synthesise the available evidence and establish the risk of myocardial infarction (MI) among HIV+ compared with uninfected individuals. We also examined MI risk within subgroups of HIV+ individuals according to exposure to combination antiretroviral therapy (ART), ART class/regimen, CD4 cell count and plasma viral load (pVL) levels.
Design: Systematic review and meta-analysis.
Data sources: We searched MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials and Cochrane Database of Systematic Reviews until 18 July 2018. Furthermore, we scanned recent HIV conference abstracts (CROI, IAS/AIDS) and bibliographies of relevant articles.
Eligibility criteria: Original studies published after December 1999 and reporting comparative data relating to the rate of MI among HIV+ individuals were included.
Data extraction and synthesis: Two reviewers working in duplicate, independently extracted data. Data were pooled using random-effects meta-analysis and reported as relative risk (RR) with 95% CI.
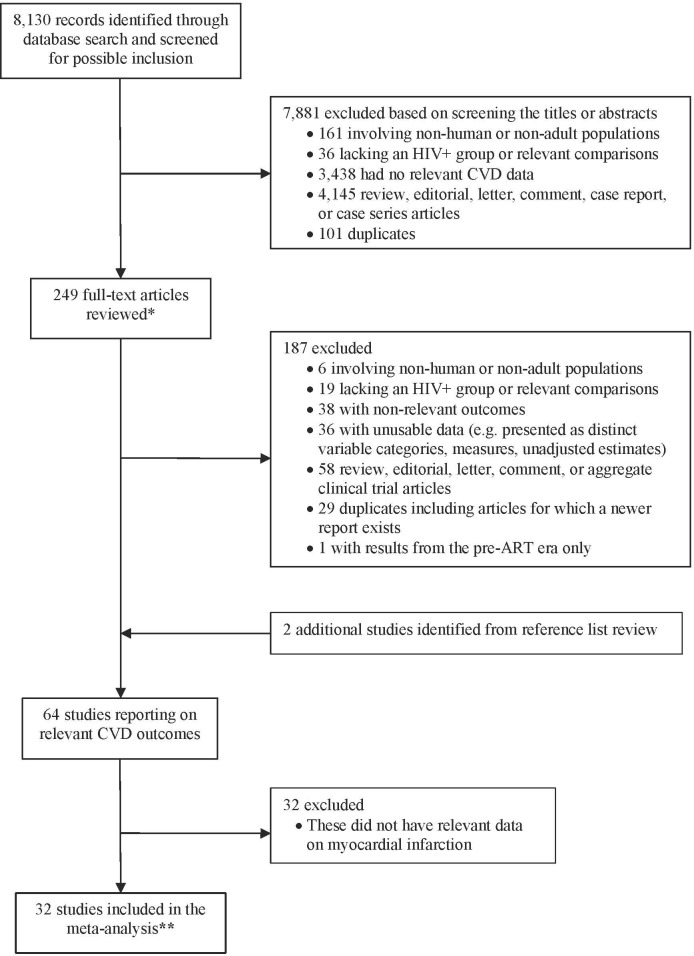
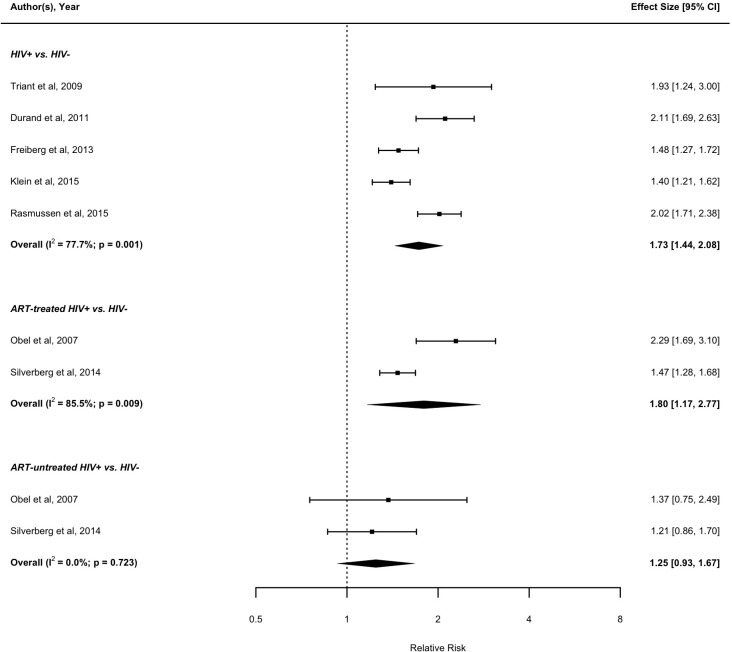
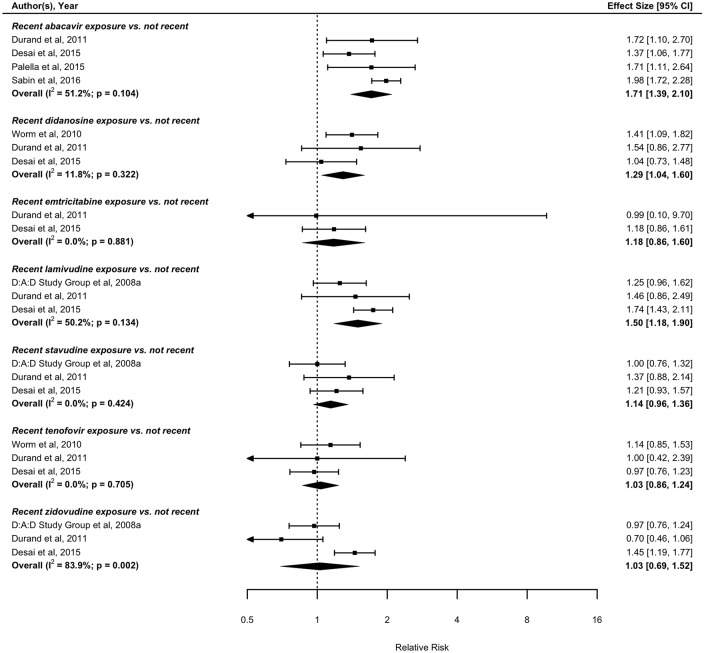
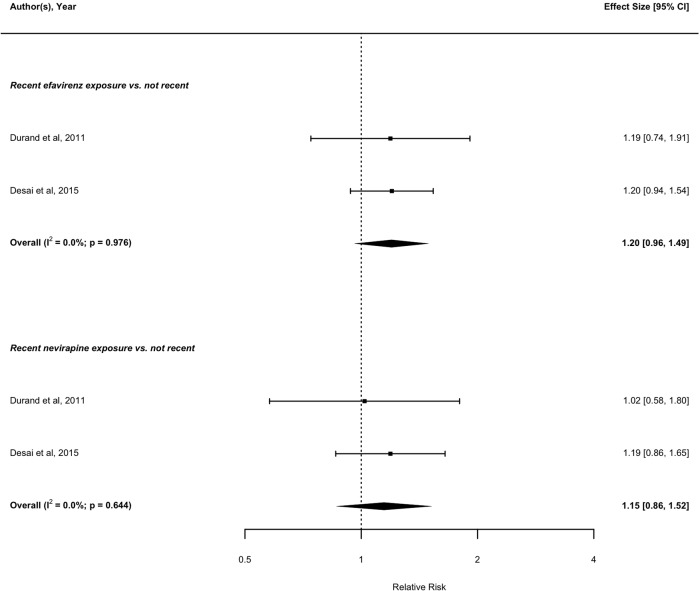
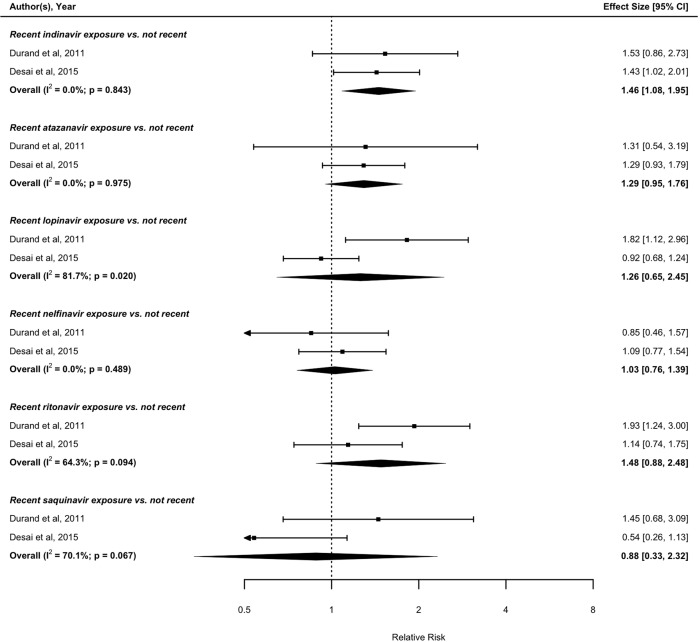
Results: Thirty-two of the 8130 identified records were included in the review. The pooled RR suggests that HIV+ individuals have a greater risk of MI compared with uninfected individuals (RR: 1.73; 95% CI 1.44 to 2.08). Depending on risk stratification, there was moderate variation according to ART uptake (RR, ART-treated=1.80; 95% CI 1.17 to 2.77; ART-untreated HIV+ individuals: 1.25; 95% CI 0.93 to 1.67, both relative to uninfected individuals). We found low CD4 count, high pVL and certain ART characteristics including cumulative ART exposure, any/cumulative use of protease inhibitors as a class, and exposure to specific ART drugs (eg, abacavir) to be importantly associated with a greater MI risk.
Conclusions: Our results indicate that HIV infection, low CD4, high pVL, cumulative ART use in general including certain exposure to specific ART class/regimen are associated with increased risk of MI. The association with cumulative ART may be an index of the duration of HIV infection with its attendant inflammation, and not entirely the effect of cumulative exposure to ART per se.
Prospero registration number: CRD42014012977.
Keywords: Cardiovascular disease; Combination antiretroviral therapy (ART); HIV; Meta-analysis; Myocardial infarction; Relative risk; Systematic review.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials