

Molecular and Microbial Microenvironments in Chronically Diseased Lungs Associated with Cystic Fibrosis
- PMID: 31551401
- PMCID: PMC6759567
- DOI: 10.1128/mSystems.00375-19
Molecular and Microbial Microenvironments in Chronically Diseased Lungs Associated with Cystic Fibrosis
Abstract
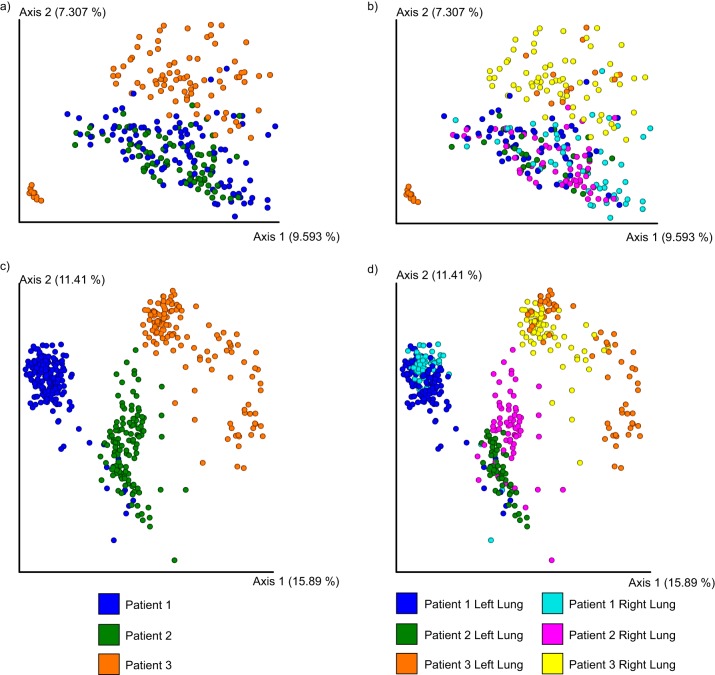
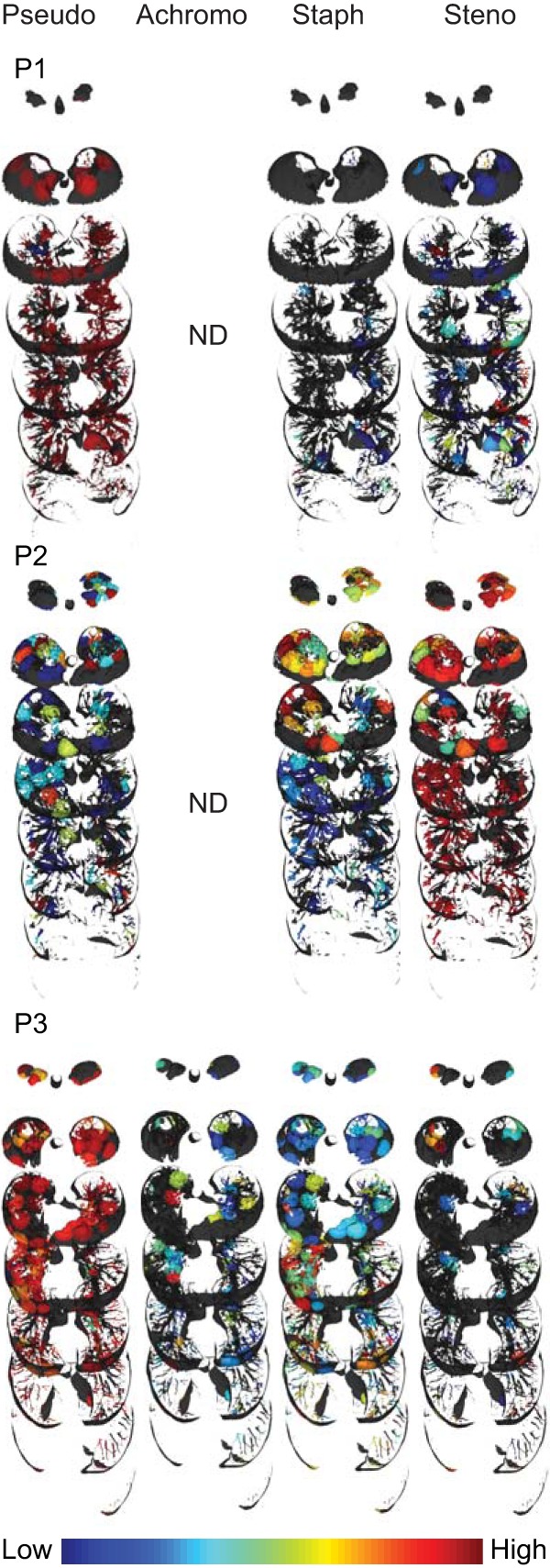
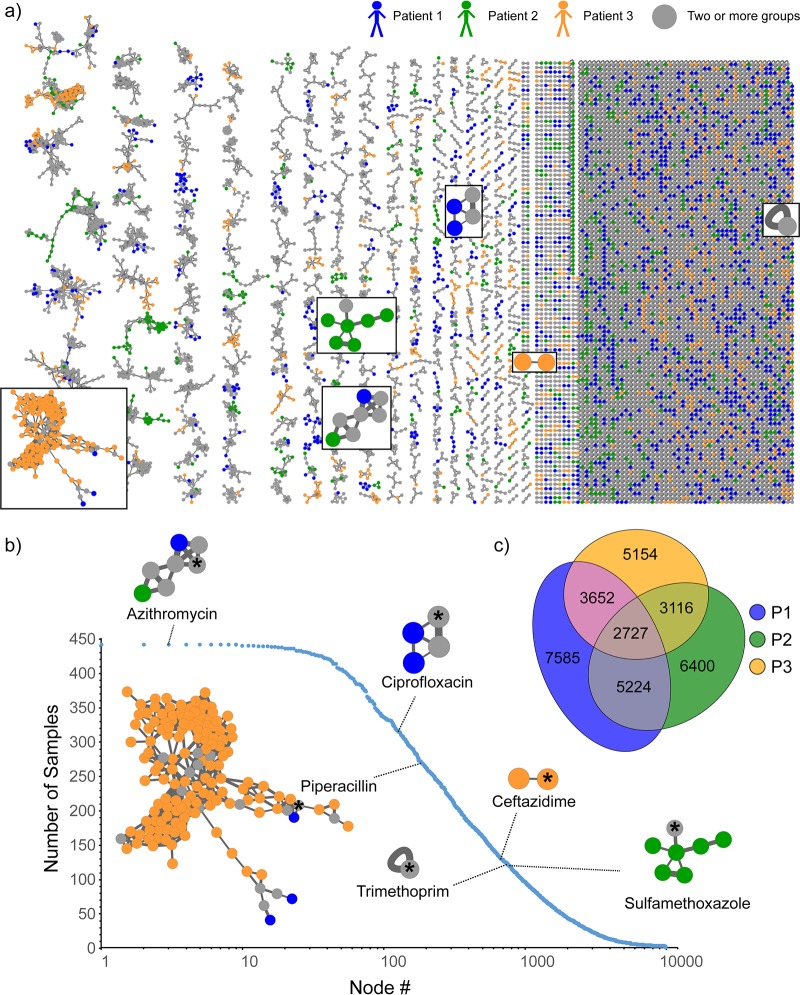
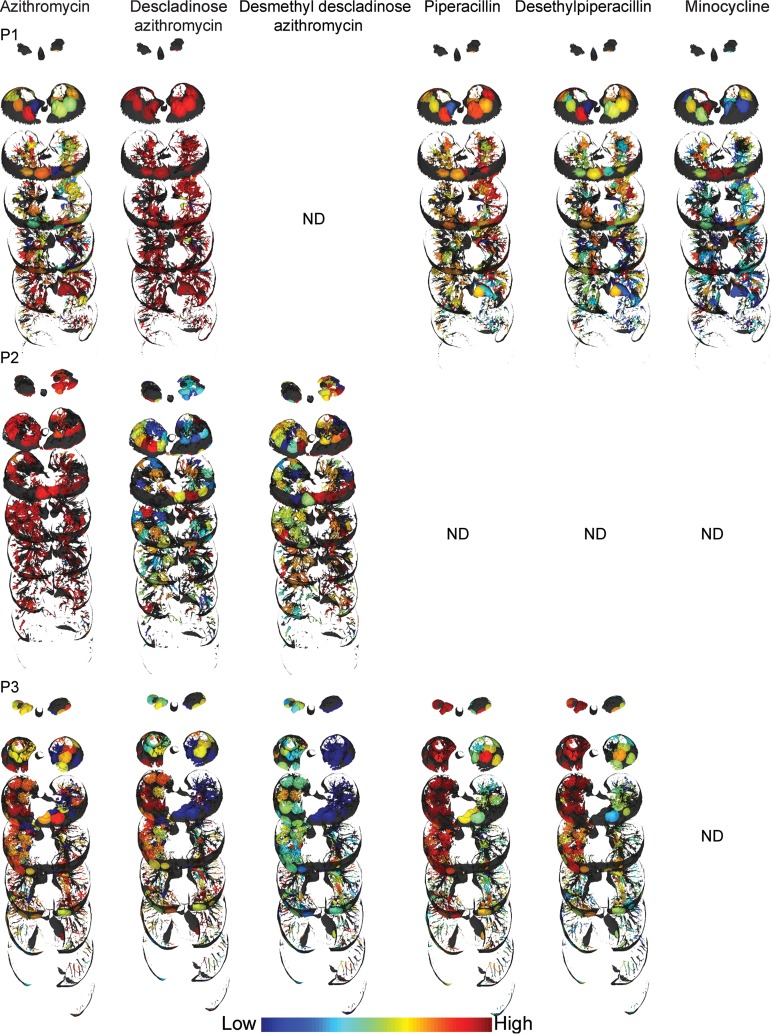
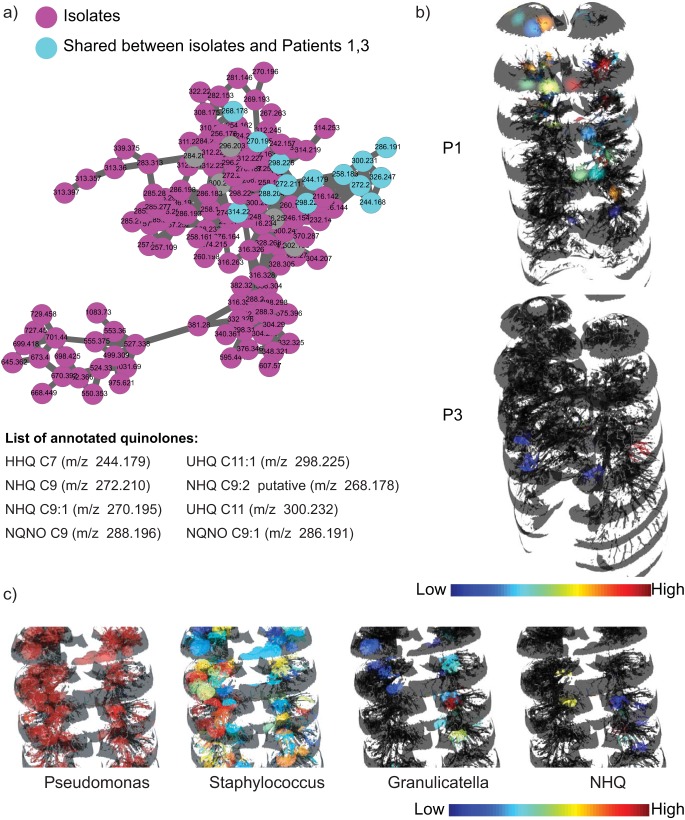
To visualize the personalized distributions of pathogens and chemical environments, including microbial metabolites, pharmaceuticals, and their metabolic products, within and between human lungs afflicted with cystic fibrosis (CF), we generated three-dimensional (3D) microbiome and metabolome maps of six explanted lungs from three cystic fibrosis patients. These 3D spatial maps revealed that the chemical environments differ between patients and within the lungs of each patient. Although the microbial ecosystems of the patients were defined by the dominant pathogen, their chemical diversity was not. Additionally, the chemical diversity between locales in the lungs of the same individual sometimes exceeded interindividual variation. Thus, the chemistry and microbiome of the explanted lungs appear to be not only personalized but also regiospecific. Previously undescribed analogs of microbial quinolones and antibiotic metabolites were also detected. Furthermore, mapping the chemical and microbial distributions allowed visualization of microbial community interactions, such as increased production of quorum sensing quinolones in locations where Pseudomonas was in contact with Staphylococcus and Granulicatella, consistent with in vitro observations of bacteria isolated from these patients. Visualization of microbe-metabolite associations within a host organ in early-stage CF disease in animal models will help elucidate the complex interplay between the presence of a given microbial structure, antibiotics, metabolism of antibiotics, microbial virulence factors, and host responses.IMPORTANCE Microbial infections are now recognized to be polymicrobial and personalized in nature. Comprehensive analysis and understanding of the factors underlying the polymicrobial and personalized nature of infections remain limited, especially in the context of the host. By visualizing microbiomes and metabolomes of diseased human lungs, we reveal how different the chemical environments are between hosts that are dominated by the same pathogen and how community interactions shape the chemical environment or vice versa. We highlight that three-dimensional organ mapping methods represent hypothesis-building tools that allow us to design mechanistic studies aimed at addressing microbial responses to other microbes, the host, and pharmaceutical drugs.
Keywords: GNPS; Pseudomonas; Stenotrophomonas; antibiotic distribution; cystic fibrosis; metabolomics; microbiome; spatial mapping.
Copyright © 2019 Melnik et al.
Figures
References
-
- Laxminarayan R, Duse A, Wattal C, Zaidi AK, Wertheim HF, Sumpradit N, Vlieghe E, Hara GL, Gould IM, Goossens H, Greko C, So AD, Bigdeli M, Tomson G, Woodhouse W, Ombaka E, Peralta AQ, Qamar FN, Mir F, Kariuki S, Bhutta ZA, Coates A, Bergstrom R, Wright GD, Brown ED, Cars O. 2013. Antibiotic resistance-the need for global solutions. Lancet Infect Dis 13:1057–1098. doi:10.1016/S1473-3099(13)70318-9. - DOI - PubMed
-
- Mollenkopf DF, Stull JW, Mathys DA, Bowman AS, Feicht SM, Grooters SV, Daniels JB, Wittum TE. 2017. Carbapenemase-producing Enterobacteriaceae recovered from the environment of a swine farrow-to-finish operation in the United States. Antimicrob Agents Chemother 61:e01298-16. doi:10.1128/AAC.01298-16. - DOI - PMC - PubMed
