

Chronic Kidney Disease as a Risk Factor for Heart Failure With Preserved Ejection Fraction: A Focus on Microcirculatory Factors and Therapeutic Targets
- PMID: 31551803
- PMCID: PMC6737277
- DOI: 10.3389/fphys.2019.01108
Chronic Kidney Disease as a Risk Factor for Heart Failure With Preserved Ejection Fraction: A Focus on Microcirculatory Factors and Therapeutic Targets
Abstract
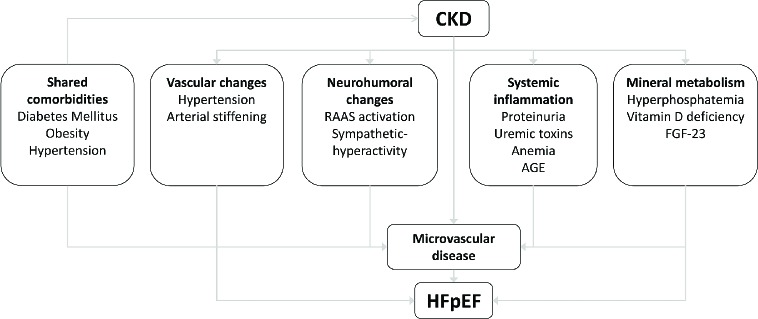
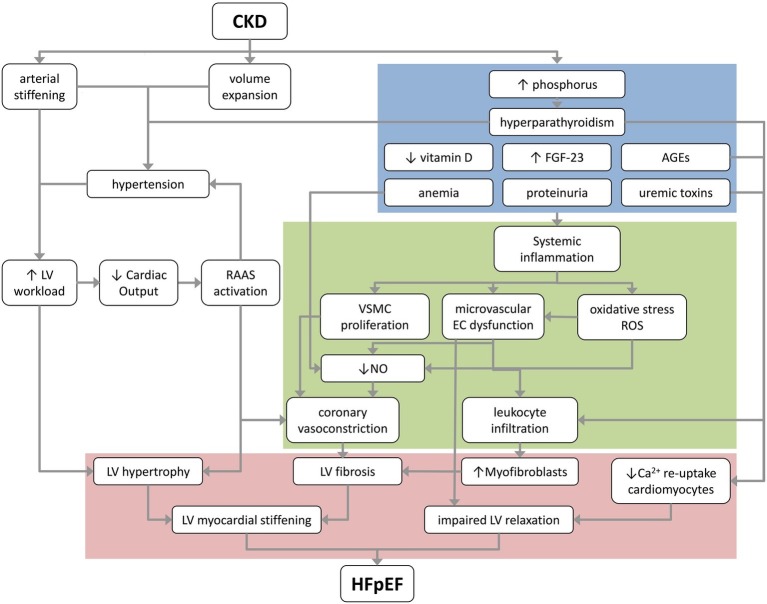
Heart failure (HF) and chronic kidney disease (CKD) co-exist, and it is estimated that about 50% of HF patients suffer from CKD. Although studies have been performed on the association between CKD and HF with reduced ejection fraction (HFrEF), less is known about the link between CKD and heart failure with preserved ejection fraction (HFpEF). Approximately, 50% of all patients with HF suffer from HFpEF, and this percentage is projected to rise in the coming years. Therapies for HFrEF are long established and considered quite successful. In contrast, clinical trials for treatment of HFpEF have all shown negative or disputable results. This is likely due to the multifactorial character and the lack of pathophysiological knowledge of HFpEF. The typical co-existence of HFpEF and CKD is partially due to common underlying comorbidities, such as hypertension, dyslipidemia and diabetes. Macrovascular changes accompanying CKD, such as hypertension and arterial stiffening, have been described to contribute to HFpEF development. Furthermore, several renal factors have a direct impact on the heart and/or coronary microvasculature and may underlie the association between CKD and HFpEF. These factors include: (1) activation of the renin-angiotensin-aldosterone system, (2) anemia, (3) hypercalcemia, hyperphosphatemia and increased levels of FGF-23, and (4) uremic toxins. This review critically discusses the above factors, focusing on their potential contribution to coronary dysfunction, left ventricular stiffening, and delayed left ventricular relaxation. We further summarize the directions of novel treatment options for HFpEF based on the contribution of these renal drivers.
Keywords: HFpEF; chronic kidney disease; heart failure; microcirculation; therapy; vasculature.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous