

T Cells Are Dominant Population in Human Abdominal Aortic Aneurysms and Their Infiltration in the Perivascular Tissue Correlates With Disease Severity
- PMID: 31552015
- PMCID: PMC6736986
- DOI: 10.3389/fimmu.2019.01979
T Cells Are Dominant Population in Human Abdominal Aortic Aneurysms and Their Infiltration in the Perivascular Tissue Correlates With Disease Severity
Abstract
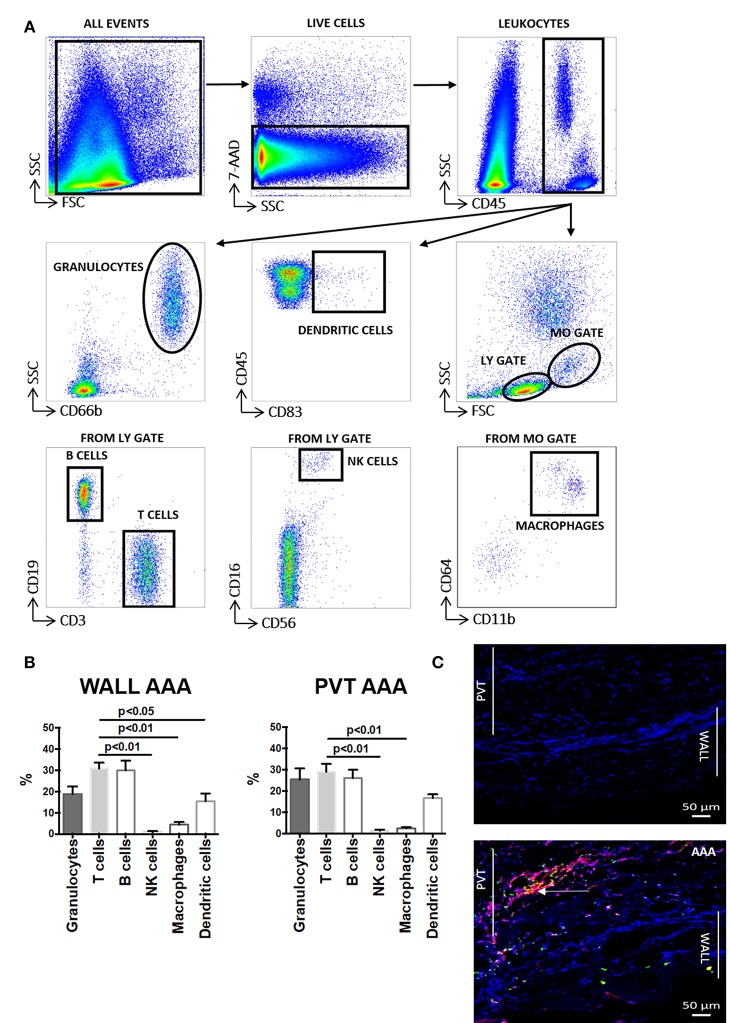
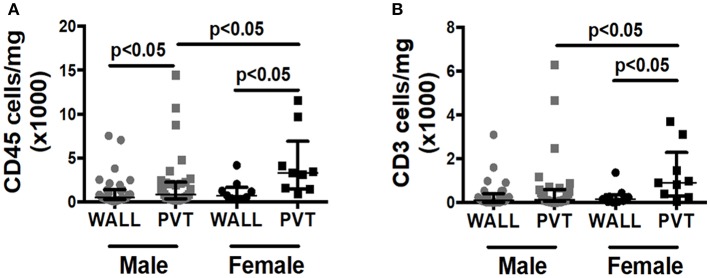
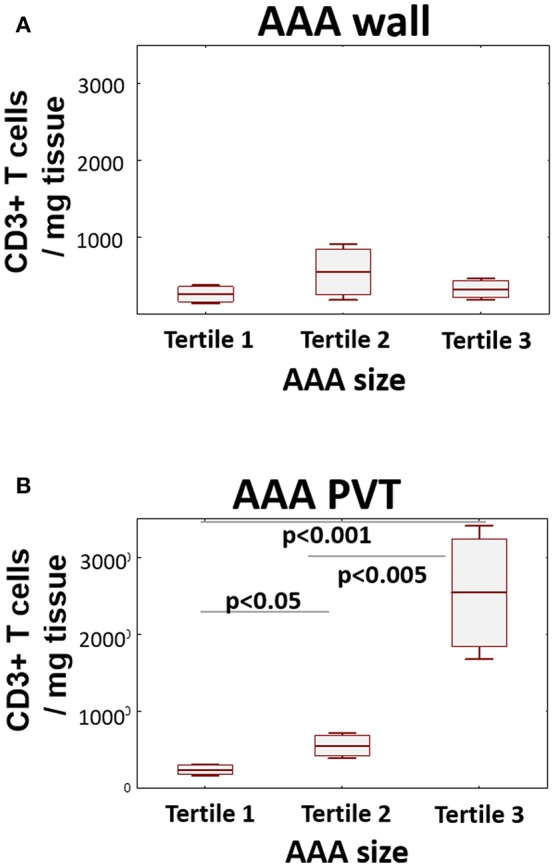
Abdominal Aortic Aneurysm (AAA) is a major cause of cardiovascular mortality. Adverse changes in vascular phenotype act in concert with chronic inflammation to promote AAA progression. Perivascular adipose tissue (PVAT) helps maintain vascular homeostasis but when inflamed and dysfunctional, can also promote vascular pathology. Previous studies suggested that PVAT may be an important site of vascular inflammation in AAA; however, a detailed assessment of leukocyte populations in human AAA, their anatomic location in the vessel wall and correlation to AAA size remain undefined. Accordingly, we performed in depth immunophenotyping of cells infiltrating the pathologically altered perivascular tissue (PVT) and vessel wall in AAA samples at the site of maximal dilatation (n = 51 patients). Flow cytometry revealed that T cells, rather than macrophages, are the major leukocyte subset in AAA and that their greatest accumulations occur in PVT. Both CD4+ and CD8+ T cell populations are highly activated in both compartments, with CD4+ T cells displaying the highest activation status within the AAA wall. Finally, we observed a positive relationship between T cell infiltration in PVT and AAA wall. Interestingly, only PVT T cell infiltration was strongly related to tertiles of AAA size. In summary, this study highlights an important role for PVT as a reservoir of T lymphocytes and potentially as a key site in modulating the underlying inflammation in AAA.
Keywords: T cell; abdominal aortic aneurysm; inflammation; macrophages; perivascular adipose tissue.
Figures

Similar articles
-
Inflammatory cells, ceramides, and expression of proteases in perivascular adipose tissue adjacent to human abdominal aortic aneurysms.J Vasc Surg. 2017 Apr;65(4):1171-1179.e1. doi: 10.1016/j.jvs.2015.12.056. Epub 2016 Mar 6. J Vasc Surg. 2017. PMID: 26960947
-
Inflammatory Gene Expression of Human Perivascular Adipose Tissue in Abdominal Aortic Aneurysms.Eur J Vasc Endovasc Surg. 2021 Jun;61(6):1008-1016. doi: 10.1016/j.ejvs.2021.02.034. Epub 2021 Apr 12. Eur J Vasc Endovasc Surg. 2021. PMID: 33858751
-
Genome-Wide Expression Profiling Unveils Autoimmune Response Signatures in the Perivascular Adipose Tissue of Abdominal Aortic Aneurysm.Arterioscler Thromb Vasc Biol. 2019 Feb;39(2):237-249. doi: 10.1161/ATVBAHA.118.311803. Arterioscler Thromb Vasc Biol. 2019. PMID: 30567485
-
Understanding the Potential Function of Perivascular Adipose Tissue in Abdominal Aortic Aneurysms: Current Research Status and Future Expectation.Curr Med Chem. 2023;30(40):4554-4568. doi: 10.2174/0929867330666221202142234. Curr Med Chem. 2023. PMID: 36476437 Review.
-
B lymphocytes in abdominal aortic aneurysms.Atherosclerosis. 2015 Sep;242(1):311-7. doi: 10.1016/j.atherosclerosis.2015.07.036. Epub 2015 Jul 21. Atherosclerosis. 2015. PMID: 26233918 Review.
Cited by
-
Activated invariant natural killer T cells infiltrate aortic tissue as key participants in abdominal aortic aneurysm pathology.Immunology. 2021 Dec;164(4):792-802. doi: 10.1111/imm.13401. Epub 2021 Aug 19. Immunology. 2021. PMID: 34379797 Free PMC article.
-
Identification of core cuprotosis-correlated biomarkers in abdominal aortic aneurysm immune microenvironment based on bioinformatics.Front Immunol. 2023 Apr 17;14:1138126. doi: 10.3389/fimmu.2023.1138126. eCollection 2023. Front Immunol. 2023. PMID: 37138870 Free PMC article.
-
POU class 2 homeobox associating factor 1 (POU2AF1) participates in abdominal aortic aneurysm enlargement based on integrated bioinformatics analysis.Bioengineered. 2021 Dec;12(1):8980-8993. doi: 10.1080/21655979.2021.1990822. Bioengineered. 2021. PMID: 34637689 Free PMC article.
-
Reversal of elastase-induced abdominal aortic aneurysm following the delivery of nanoparticle-based pentagalloyl glucose (PGG) is associated with reduced inflammatory and immune markers.Eur J Pharmacol. 2021 Nov 5;910:174487. doi: 10.1016/j.ejphar.2021.174487. Epub 2021 Sep 10. Eur J Pharmacol. 2021. PMID: 34516951 Free PMC article.
-
Differential Expression Analyses on Human Aortic Tissue Reveal Novel Genes and Pathways Associated With Abdominal Aortic Aneurysm Onset and Progression.J Am Heart Assoc. 2024 Dec 17;13(24):e036082. doi: 10.1161/JAHA.124.036082. Epub 2024 Dec 10. J Am Heart Assoc. 2024. PMID: 39655704 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials