

Association of Frailty With 30-Day Outcomes for Acute Myocardial Infarction, Heart Failure, and Pneumonia Among Elderly Adults
- PMID: 31553402
- PMCID: PMC6763977
- DOI: 10.1001/jamacardio.2019.3511
Association of Frailty With 30-Day Outcomes for Acute Myocardial Infarction, Heart Failure, and Pneumonia Among Elderly Adults
Abstract
Importance: The addition of a claims-based frailty metric to traditional comorbidity-based risk-adjustment models for acute myocardial infarction (AMI), heart failure (HF), and pneumonia improves the prediction of 30-day mortality and readmission. This may have important implications for hospitals that tend to care for frail populations and participate in Centers for Medicare & Medicaid Services value-based payment programs, which use these risk-adjusted metrics to determine reimbursement.
Objective: To determine whether the addition of frailty measures to traditional comorbidity-based risk-adjustment models improved prediction of outcomes for patients with AMI, HF, and pneumonia.
Design, setting, and participants: A nationwide cohort study included Medicare fee-for-service beneficiaries 65 years and older in the United States between January 1 and December 1, 2016. Analysis began August 2018.
Main outcomes and measures: Rates of mortality within 30 days of admission and 30 days of discharge, as well as 30-day readmission rates by frailty group. We evaluated the incremental effect of adding the Hospital Frailty Risk Score (HFRS) to current comorbidity-based risk-adjustment models for 30-day outcomes across all conditions.
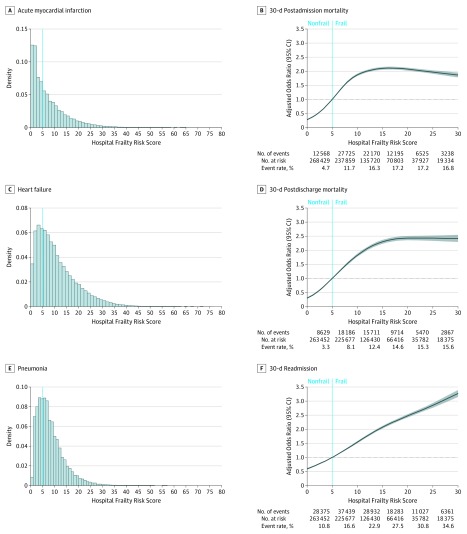
Results: For 785 127 participants, there were 166 200 hospitalizations [21.2%] for AMI, 348 619 [44.4%] for HF, and 270 308 [34.4%] for pneumonia. The mean (SD) age at the time of hospitalization was 79.2 (8.9) years; 656 315 (83.6%) were white and 402 639 (51.3%) were women. The mean (SD) HFRS was 7.3 (7.4) for patients with AMI, 10.8 (8.3) for patients with HF, and 8.2 (5.7) for patients with pneumonia. Among patients hospitalized for AMI, an HFRS more than 15 (compared with an HFRS <5) was associated with a higher risk of 30-day postadmission mortality (adjusted odds ratio [aOR], 3.6; 95% CI, 3.4-3.8), 30-day postdischarge mortality (aOR, 4.0; 95% CI, 3.7-4.3), and 30-day readmission (aOR, 3.0; 95% CI, 2.9-3.1) after multivariable adjustment for age, sex, race, and comorbidities. Similar patterns were observed for patients hospitalized with HF (30-day postadmission mortality: aOR, 3.5; 95% CI, 3.4-3.7; 30-day postdischarge mortality: aOR, 3.5; 95% CI, 3.3-3.6; and 30-day readmission: aOR, 2.9; 95% CI, 2.8-3.0) and among patients with pneumonia (30-day postadmission mortality: aOR, 2.5; 95% CI, 2.3-2.6; 30-day postdischarge mortality: aOR, 3.0; 95% CI, 2.9-3.2; and 30-day readmission: aOR, 2.8; 95% CI, 2.7-2.9). The addition of HFRS to traditional comorbidity-based risk-prediction models improved discrimination to predict outcomes for all 3 conditions.
Conclusions and relevance: Among Medicare fee-for-service beneficiaries, frailty as measured by the HFRS was associated with mortality and readmissions among patients hospitalized for AMI, HF, or pneumonia. The addition of HFRS to traditional comorbidity-based risk-prediction models improved the prediction of outcomes for all 3 conditions.
Conflict of interest statement
Figures
Comment in
-
Frailty Measurement Using Administrative Data in Older Patients With Cardiovascular Disease.JAMA Cardiol. 2020 Aug 1;5(8):967-968. doi: 10.1001/jamacardio.2020.1552. JAMA Cardiol. 2020. PMID: 32432688 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
