

Health Risks and Interventions in Exertional Heat Stress
- PMID: 31554541
- PMCID: PMC6783627
- DOI: 10.3238/arztebl.2019.0537
Health Risks and Interventions in Exertional Heat Stress
Abstract
Background: With climate change, heat waves are expected to become more frequent in the near future. Already, on average more than 25 000 "heat deaths" are estimated to occur in Europe every year. However, heat stress and heat illnesses arise not just when ambient temperatures are high. Physical exertion increases heat production within the organism many times over; if not enough heat is lost, there is a risk of exertional heat stress. This review article discusses contributing factors, at-risk groups, and the diagnosis and treatment of heat illnesses.
Methods: A selective literature search was carried out on PubMed. Current guidelines and expert recommendations were also included.
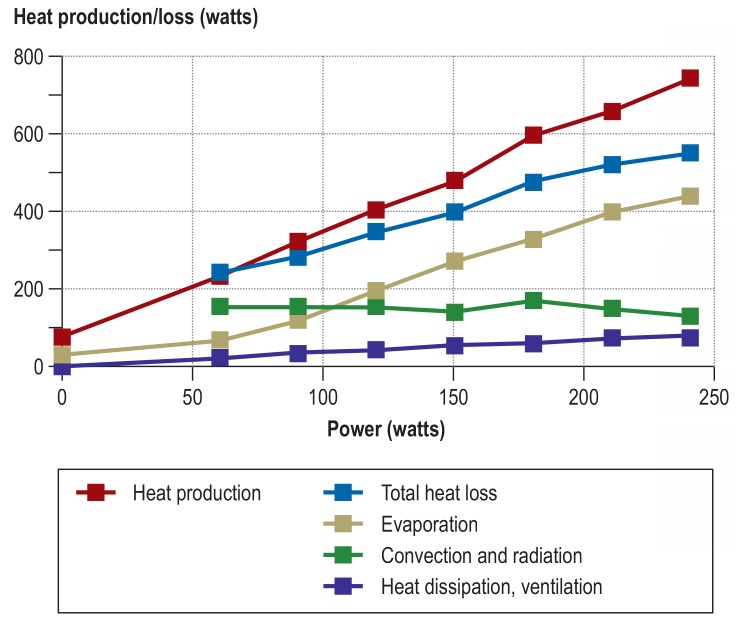
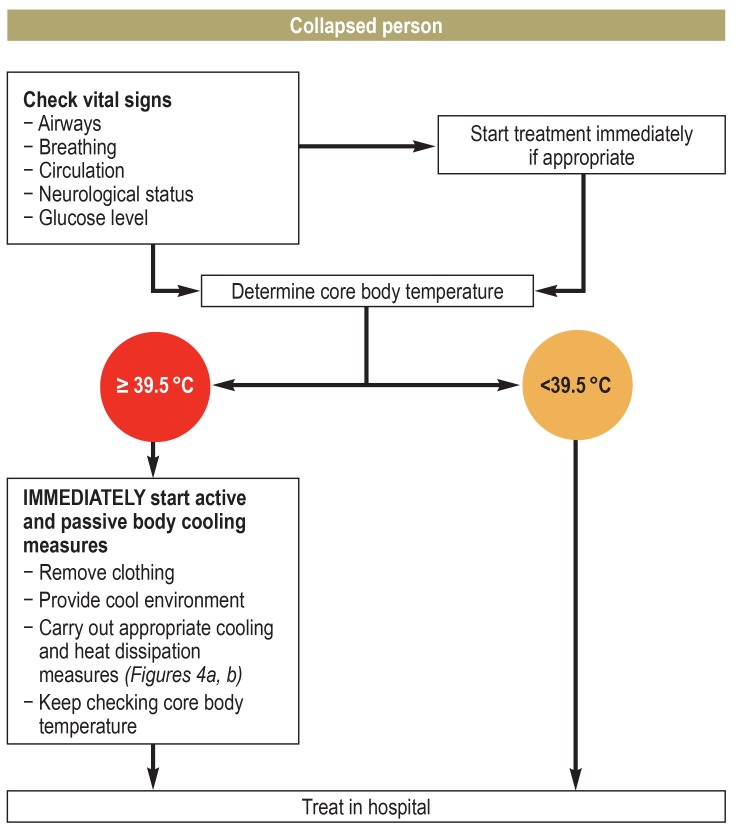
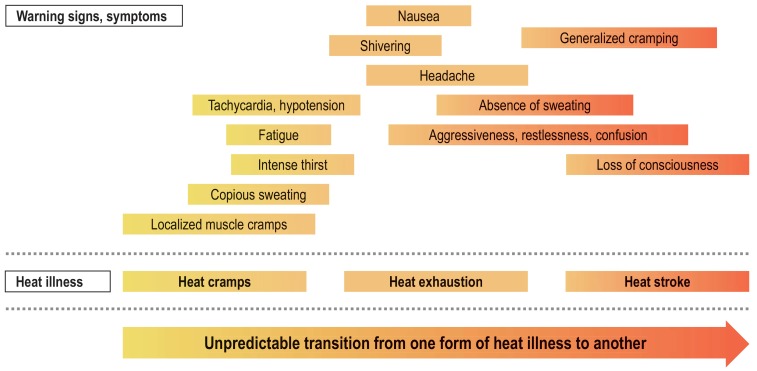
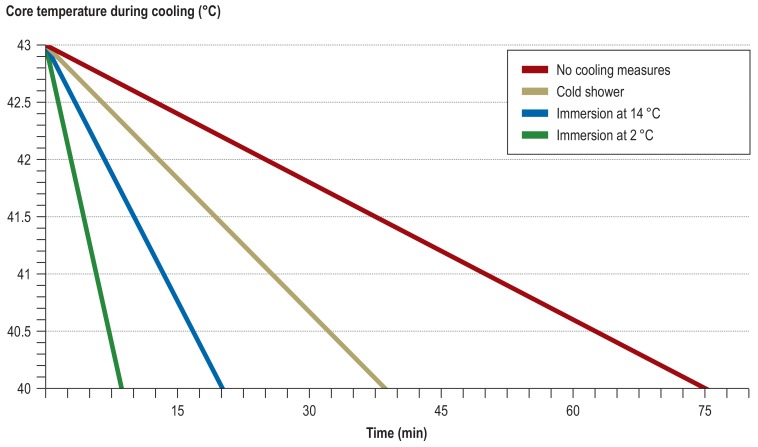
Results: Apart from muscular heat production (>70% of converted energy), there are other factors that singly or in combination can give rise to heat stress: clothing, climate/acclimatization, and individual factors. Through its insulating properties, clothing reduces the evaporation of sweat (the most effective physiological cooling mechanism). A sudden heat wave, or changing the climate zone (as with air travel), increases the risk of a heat-related health event. Overweight, low fitness level, acute infections, illness, dehydration, and other factors also reduce heat tolerance. In addition to children, older people are particularly at risk because of their reduced physiological adaptability, (multi-)morbidity, and intake of prescription drugs. A heat illness can progress suddenly to life-threatening heat stroke. Successful treatment depends on rapid diagnosis and cooling the body down as quickly as possible. The aim is to reduce core body temperature to <40 °C within 30 minutes.
Conclusion: Immediately effective cooling interventions are the only causal treatment for heat stroke. Time once lost cannot be made up. Prevention (acclimatization, reduced exposure, etc.) and terminating the heat stress in good time (e.g., stopping work) are better than any cure.
Figures

References
-
- Leyk D. Körperliche Arbeit bei Hitzestress: Eine oft unterschätzte Belastung und Gefahr. Wehrmed Mschr. 2018;62:354–356.
-
- Bedno SA, Li Y, Han W, et al. Exertional heat illness among overweight US. Army recruits in basic training. Aviat Space Environ Med. 2010;81:107–111. - PubMed
-
- Epstein Y, Moran DS, Shapiro Y. Pandolf KB, Burr RE, editors. Exertional heatstroke in the Israeli defence forces Textbooks of military medicine. Volume 1: Medical aspects of harsh environments. Falls Church: Office of the Surgeon General. 2001:281–292.
-
- Israel S. Lehrbuch der Sportmedizin. 4th edition. Heidelberg Barth: 1999. Thermoregulation und Wasserhaushalt In: Badtke G, Bittmann F (eds.): pp. 268–276.
-
- Galloway SD, Maughan RJ. Effects of ambient temperature on the capacity to perform prolonged cycle exercise in man. Med Sci Sports Exerc. 1997;29:1240–1249. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical