

Progressive multifocal leukoencephalopathy: A 25-year retrospective cohort study
- PMID: 31554669
- PMCID: PMC6814409
- DOI: 10.1212/NXI.0000000000000618
Progressive multifocal leukoencephalopathy: A 25-year retrospective cohort study
Abstract
Objective: To characterize the risk factors, clinical course, and treatment of patients with progressive multifocal leukoencephalopathy (PML) diagnosed and followed over a 25-year epoch at 2 academic hospitals.
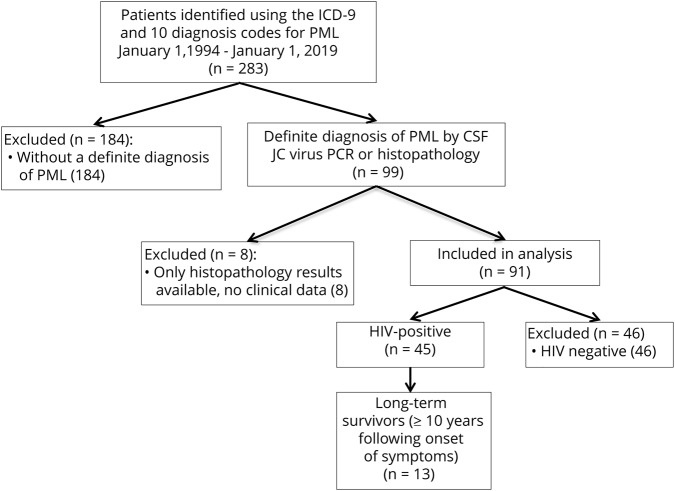
Methods: Patients with a definite diagnosis of PML were identified by positive CSF PCR for JC virus or histopathology between January 1, 1994, and January 1, 2019. Demographic and PML-specific variables were recorded on symptomatic presentation and at follow-up, including risk factors, clinical outcome, neuroimaging findings, and modified Rankin Scale (mRS) score at last follow-up.
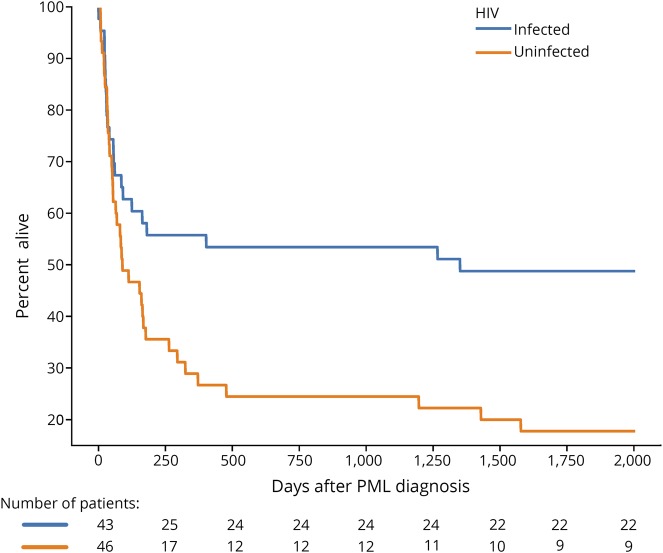
Results: There were 91 patients with confirmed PML. HIV infection was the most common risk factor, identified in 49% (n = 45). Other frequent risk factors included lymphoma, leukemia, or myelodysplasia, identified in 31% of patients (n = 28); exposure to chemotherapeutic medications (30%, n = 27); and exposure to monoclonal antibody therapies (19%, n = 17). Thirty percent of the cohort was alive at the time of censoring, with a median mRS of 2 points, indicating slight disability at last follow-up. Median survival following PML diagnosis in HIV-infected patients was longer than in HIV-uninfected patients (1,992 vs 101 days, p = 0.024). Forty patients survived more than 1 year after PML symptom onset, of whom 24 were HIV infected (60%). Thirteen patients survived more than 10 years after PML symptom onset, all HIV infected, of the 59 patients diagnosed before June 1, 2009, and eligible for 10-year survivor status (22%).
Conclusions: We add to the limited literature on PML by reporting its epidemiology in a large observational cohort. These parameters may be useful for future clinical trials that measure survival and clinical outcomes.
Copyright © 2019 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical