

Influence and mechanism of lung cavitation development on antiangiogenic therapy
- PMID: 31555522
- PMCID: PMC6749114
- DOI: 10.21037/tlcr.2019.07.01
Influence and mechanism of lung cavitation development on antiangiogenic therapy
Abstract
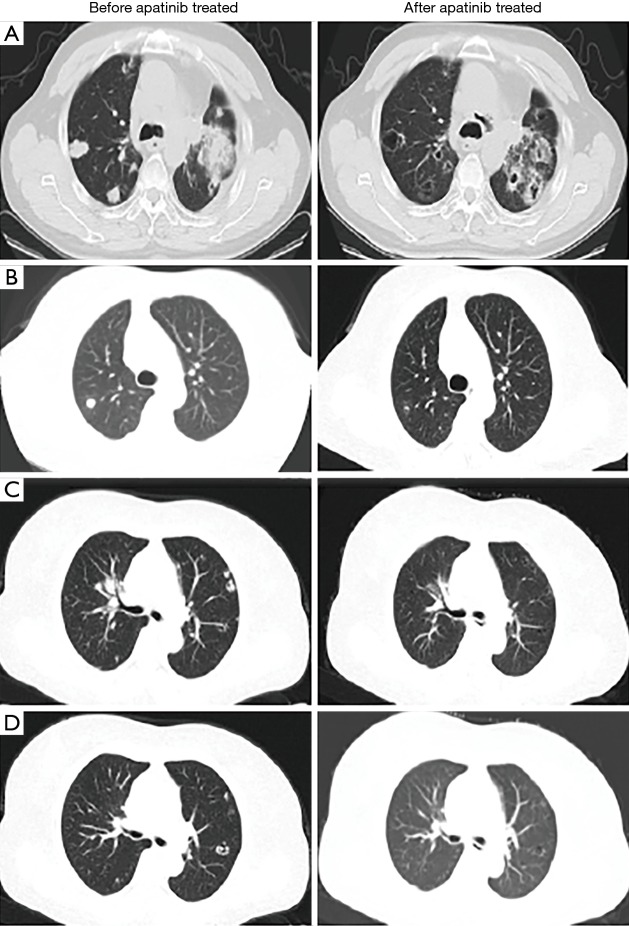
Background: Antiangiogenic agent-treated patients usually develop cavitation in their lung lesions. The clinical significance of lung cavitation development during antiangiogenic therapy has not been determined yet. Herein, we evaluated the clinical outcomes of patients who developed tumor cavitation following apatinib treatment and explored the mechanisms.
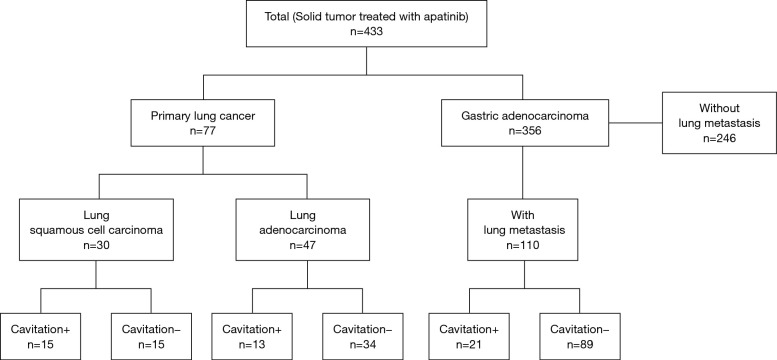
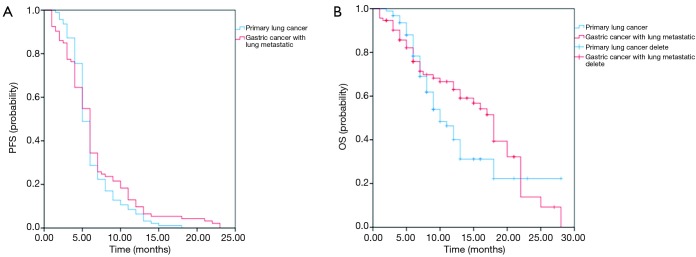
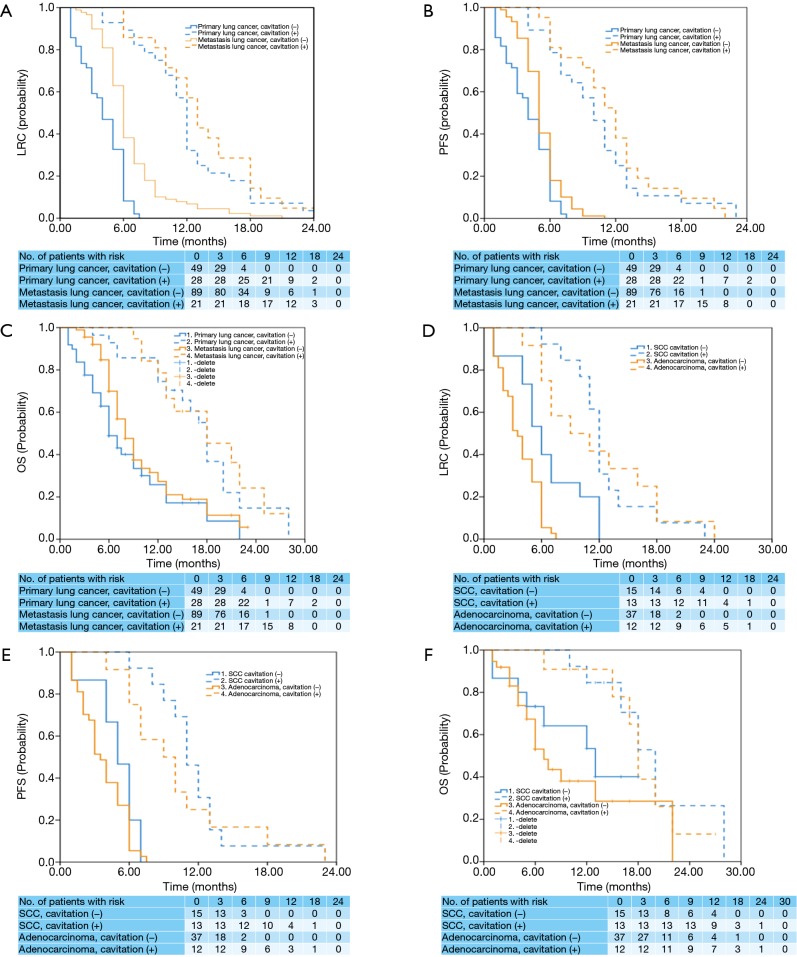
Methods: In this study (Clinical Trial No. NCT03629691), 187 patients (77 lung cancer and 110 gastric adenocarcinoma patients) who had progressed or relapsed after undergoing at least two lines of systemic therapy in accordance with the NCCN guidelines for primary or metastatic lung tumors were treated with apatinib at a dosage of 250 mg per day between February 1, 2015 and May 19, 2017. The effect of lung cavitation development on locoregional control (LRC), progression-free survival (PFS), and overall survival (OS) was analyzed with Kaplan-Meier estimates and compared with the log-rank test. Zebrafish experiments were used to study the anticancer mechanism of apatinib in different tumors. Western-blotting was used to analyze the expression of Cyclin D1, p53, HIF-α, and VEGFR before and after apatinib treatment in both normoxia and hypoxia.
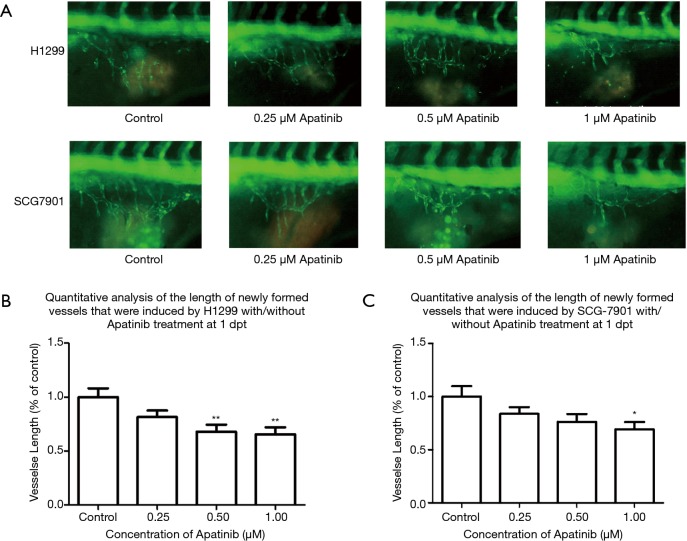
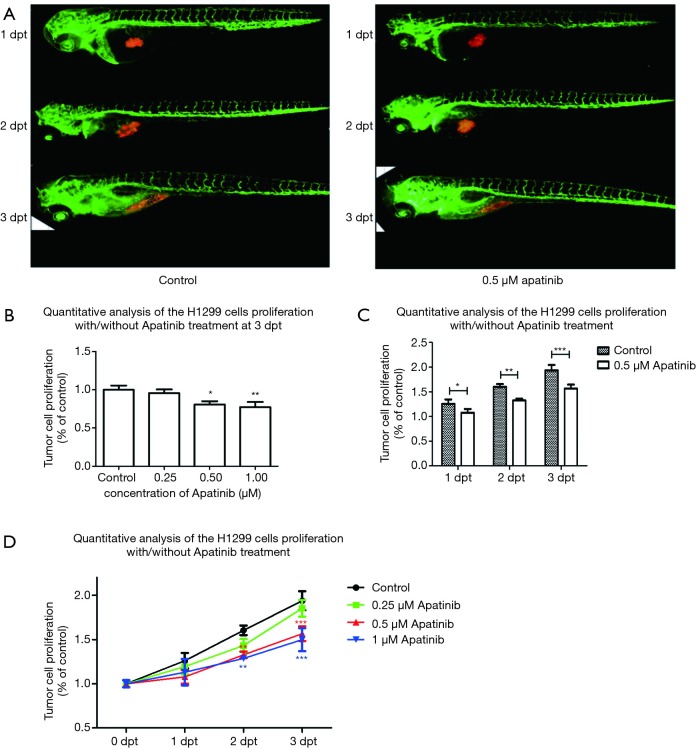
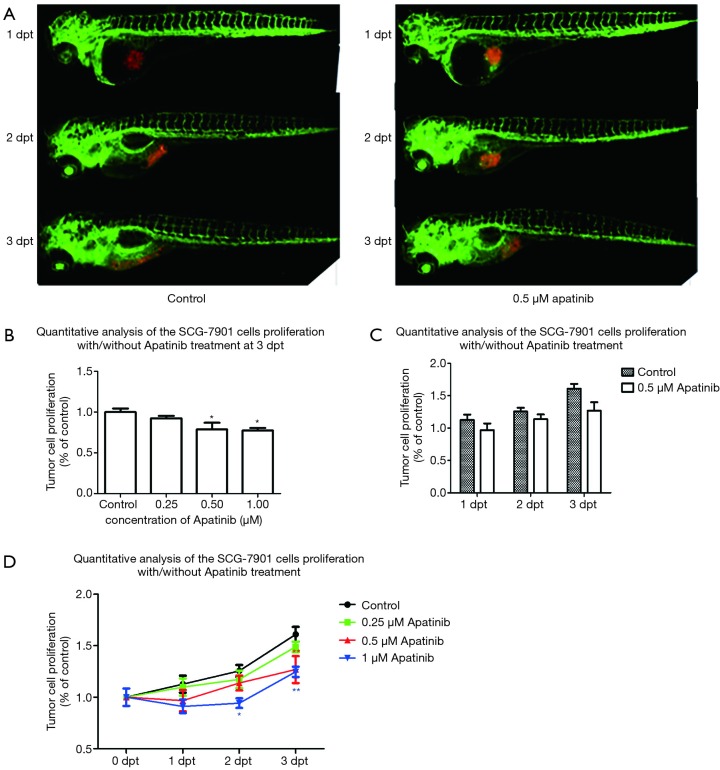
Results: Cavitation development was beneficial in patients receiving apatinib therapy regardless of whether they had primary or metastatic lung cancer. Zebrafish experiments showed that apatinib inhibited tumor growth by both suppressing vascular growth and inhibiting cell proliferation. Vascular proliferation induced by the H1299 cell lines showed higher sensitivity to apatinib than that induced by the SCG-7901 cell line. However, apatinib showed weak tumor type selectivity on cell proliferation inhibition in vivo. Under hypoxic conditions, apatinib could not inhibit the protein expression of VEGFR and HIF-α in both cell lines; however, apatinib decreased the expression of cyclin D1 and P53 significantly.
Conclusions: Lung cavitation development is common with apatinib therapy and is a potential prognostic marker. Apatinib inhibits tumor growth by both vessel growth inhibition and proliferation inhibition.
Keywords: Apatinib; anticancer mechanism; hypoxia; lung cavitation development; progression-free survival (PFS).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures

Comment in
-
What's in a (tumor) cavity?Transl Lung Cancer Res. 2020 Feb;9(1):8-9. doi: 10.21037/tlcr.2019.10.01. Transl Lung Cancer Res. 2020. PMID: 32206548 Free PMC article. No abstract available.
References
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous