

Minimal Residual Disease in Chronic Lymphocytic Leukemia: A New Goal?
- PMID: 31555576
- PMCID: PMC6727319
- DOI: 10.3389/fonc.2019.00689
Minimal Residual Disease in Chronic Lymphocytic Leukemia: A New Goal?
Abstract
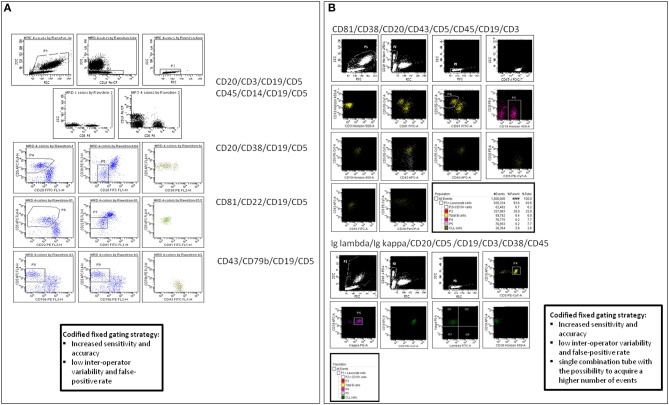
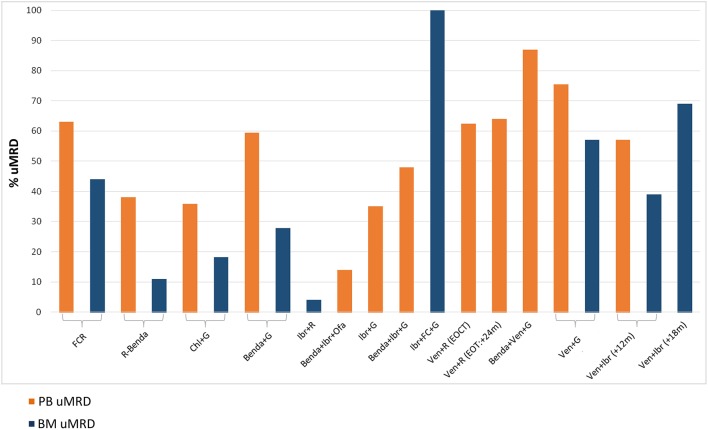
In chronic lymphocytic leukemia (CLL), there is a growing interest for minimal residual disease (MRD) monitoring, due to the availability of drug combinations capable of unprecedented complete clinical responses. The standardized and most commonly applied methods to assess MRD in CLL are based on flow cytometry (FCM) and, to a lesser extent, real-time quantitative PCR (RQ-PCR) with allele-specific oligonucleotide (ASO) primers of immunoglobulin heavy chain genes (IgH). Promising results are being obtained using droplet digital PCR (ddPCR) and next generation sequencing (NGS)-based approaches, with some advantages and a potential higher sensitivity compared to the standardized methodologies. Plasma cell-free DNA can also be explored as a more precise measure of residual disease from all different compartments, including the lymph nodes. From a clinical point of view, CLL MRD quantification has proven an independent prognostic marker of progression-free survival (PFS) and overall survival (OS) after chemoimmunotherapy as well as after allogeneic transplantation. In the era of mechanism-driven drugs, the paradigms of CLL treatment are being revolutionized, challenging the use of chemoimmunotherapy even in first-line. The continuous administration of ibrutinib single agent has led to prolonged PFS and OS in relapsed/refractory and treatment naïve CLL, including those with TP53 deletion/mutation or unmutated IGHV genes, though the clinical responses are rarely complete. More recently, chemo-free combinations of venetoclax+rituximab, venetoclax+obinutuzumab or ibrutinib+venetoclax have been shown capable of inducing undetectable MRD in the bone marrow, opening the way to protocols exploring a MRD-based duration of treatment, aiming at disease eradication. Thus, beside a durable disease control desirable particularly for older patients and/or for those with comorbidities, a MRD-negative complete remission is becoming a realistic prospect for CLL patients in an attempt to obtain a long-lasting eradication and possibly cure of the disease. Here we discuss the standardized and innovative technical approaches for MRD detection in CLL, the clinical impact of MRD monitoring in chemoimmunotherapy and chemo-free trials and the future clinical implications of MRD monitoring in CLL patients outside of clinical trials.
Keywords: chronic lymphocytic leukemia; droplet digital PCR; flow cytometry; ibrutinib; minimal residual disease; next generation sequencing; venetoclax.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous