

Dysphagia After Primary Transoral Robotic Surgery With Neck Dissection vs Nonsurgical Therapy in Patients With Low- to Intermediate-Risk Oropharyngeal Cancer
- PMID: 31556933
- PMCID: PMC6763976
- DOI: 10.1001/jamaoto.2019.2725
Dysphagia After Primary Transoral Robotic Surgery With Neck Dissection vs Nonsurgical Therapy in Patients With Low- to Intermediate-Risk Oropharyngeal Cancer
Abstract
Importance: A major goal of primary transoral robotic surgery (TORS) for oropharyngeal cancer is to optimize swallowing outcomes by personalized treatment based on pathologic staging. However, swallowing outcomes after TORS are uncertain, as are the outcomes compared with nonsurgical options.
Objectives: To estimate rates of acute dysphagia and recovery after TORS and to compare swallowing outcomes by primary treatment modality (TORS or radiotherapy).
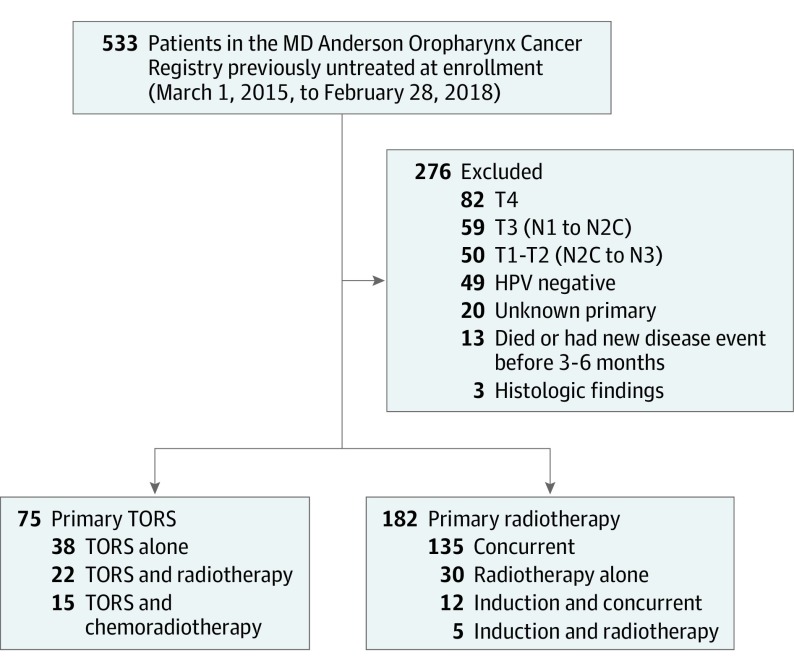
Design, setting, and participants: This case series study was a secondary analysis of prospective registry data from 257 patients enrolled from March 1, 2015, to February 28, 2018, at a single academic institution who, according to the AJCC Staging Manual, 7th edition TNM classification, had low- to intermediate-risk human papillomavirus-related oropharyngeal squamous cell carcinoma possibly resectable by TORS.
Exposure: Patients were stratified by primary treatment (75 underwent TORS and 182 received radiotherapy).
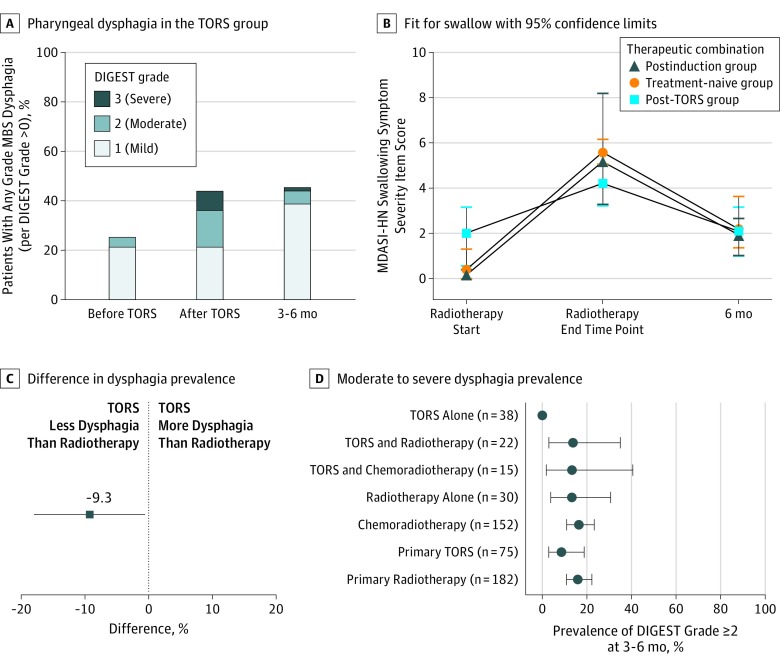
Main outcomes and measures: Modified barium swallow (MBS) studies graded per Dynamic Imaging Grade of Swallowing Toxicity (DIGEST) and the MD Anderson Symptom Inventory-Head and Neck Module (MDASI-HN) questionnaires were administered at standard intervals. Prevalence and severity of dysphagia were estimated per DIGEST before and after TORS and 3 to 6 months after treatment. Moderate-severe dysphagia (DIGEST grade ≥2) was assessed using logistic regression and compared by primary treatment group. The MDASI swallowing symptom severity item scores during and after radiotherapy were compared using generalized estimating equations by treatment status at the start of radiotherapy, after induction, and after TORS.
Results: A total of 257 patients (mean [SD] age, 59.54 [9.07] years; 222 [86.4%] male) were included in the study. Dysphagia severity (per DIGEST) was significantly worse after TORS (r = -0.63; 95% CI, -0.78 to -0.44): 17 patients (22.7%; 95% CI, 13.8%-33.8%) had moderate-severe (DIGEST grade ≥2) acute post-TORS dysphagia significantly associated with primary tumor volume (odds ratio, 1.43; 95% CI, 1.11-1.84). DIGEST improved by 3 to 6 months but remained worse than that at baseline; at 3 to 6 months, the number of patients with DIGEST grade 2 or higher dysphagia was 5 (6.7%; 95% CI, 2.2%-14.9%) after primary TORS and 29 (15.9%; 95% CI, 10.9%-22.1%) after radiotherapy. At the start of radiotherapy, MDASI swallowing symptom severity item scores were significantly worse in the post-TORS group compared with postinduction (mean [SD] change, 2.6 [1.1]) and treatment-naive (mean [SD] change, 1.7 [0.3]) patients. This result inverted at radiotherapy end, and all groups converged at 3 to 6 months.
Conclusions and relevance: Subacute swallowing outcomes were similar regardless of primary treatment modality among patients with low- to intermediate-risk oropharyngeal squamous cell carcinoma.
Conflict of interest statement
Figures
Comment in
-
Radical Radiotherapy Should Remain the Standard of Care for Carcinoma Oropharynx-Reply.JAMA Otolaryngol Head Neck Surg. 2020 May 1;146(5):505-506. doi: 10.1001/jamaoto.2020.0092. JAMA Otolaryngol Head Neck Surg. 2020. PMID: 32163110 No abstract available.
-
Radical Radiotherapy Should Remain the Standard of Care for Carcinoma Oropharynx.JAMA Otolaryngol Head Neck Surg. 2020 May 1;146(5):504-505. doi: 10.1001/jamaoto.2020.0089. JAMA Otolaryngol Head Neck Surg. 2020. PMID: 32163117 No abstract available.
References
-
- Lazarus CL, Ganz C, Ru M, Miles BA, Kotz T, Chai RL. Prospective instrumental evaluation of swallowing, tongue function, and QOL measures following transoral robotic surgery alone without adjuvant therapy. Head Neck. 2019;41(2):322-328. - PubMed
-
- Hunter KU, Schipper M, Feng FY, et al. Toxicities affecting quality of life after chemo-IMRT of oropharyngeal cancer: prospective study of patient-reported, observer-rated, and objective outcomes. Int J Radiat Oncol Biol Phys. 2013;85(4):935-940. doi: 10.1016/j.ijrobp.2012.08.030 - DOI - PMC - PubMed
