

Iron deficiency in worsening heart failure is associated with reduced estimated protein intake, fluid retention, inflammation, and antiplatelet use
- PMID: 31556953
- PMCID: PMC6868426
- DOI: 10.1093/eurheartj/ehz680
Iron deficiency in worsening heart failure is associated with reduced estimated protein intake, fluid retention, inflammation, and antiplatelet use
Abstract
Aims: Iron deficiency (ID) is common in heart failure (HF) patients and negatively impacts symptoms and prognosis. The aetiology of ID in HF is largely unknown. We studied determinants and the biomarker profile of ID in a large international HF cohort.
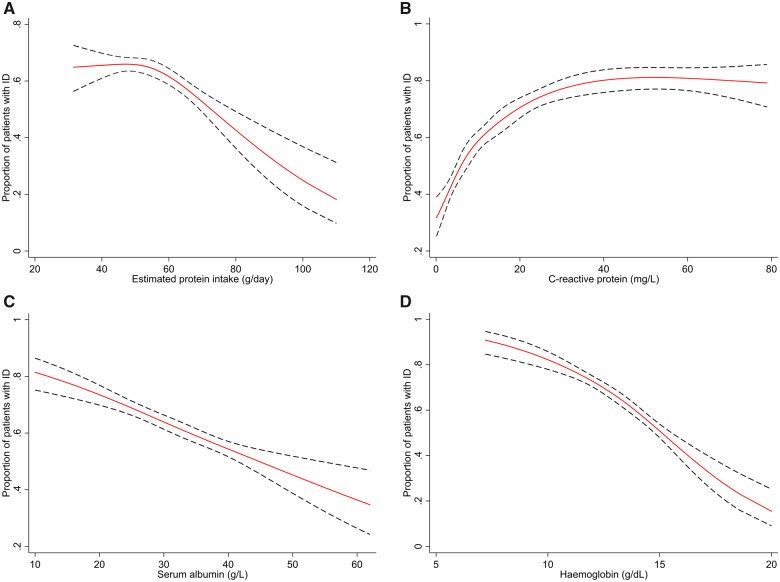
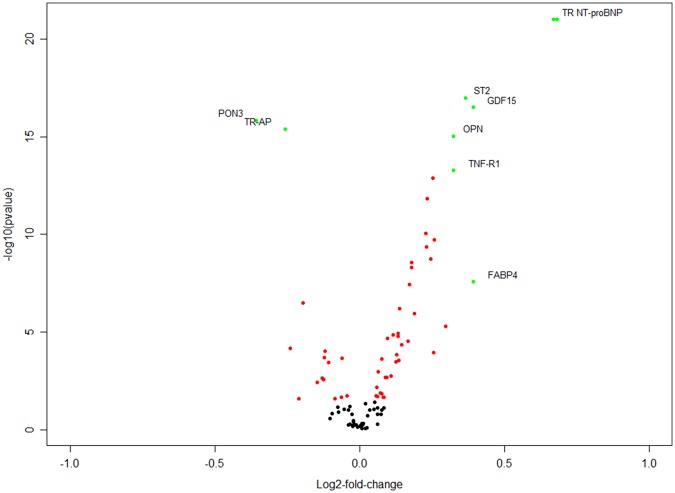
Methods and results: We studied 2357 worsening HF patients from the BIOSTAT-CHF cohort. ID was defined as transferrin saturation <20%. Univariable and multivariable logistic regression models were constructed to identify determinants for ID. We measured 92 cardiovascular markers (Olink Cardiovascular III) to establish a biomarker profile of ID. The primary endpoint was the composite of all-cause mortality and first HF rehospitalization. Mean age (±standard deviation) of all patients was 69 ± 12.0 years, 26.1% were female and median N-terminal pro B-type natriuretic peptide levels (+interquartile range) were 4305 (2360-8329) ng/L. Iron deficiency was present in 1453 patients (61.6%), with highest prevalence in females (71.1% vs. 58.3%; P < 0.001). Independent determinants of ID were female sex, lower estimated protein intake, higher heart rate, presence of peripheral oedema and orthopnoea, chronic kidney disease, lower haemoglobin, higher C-reactive protein levels, lower serum albumin levels, and P2Y12 inhibitor use (all P < 0.05). None of these determinants were sex-specific. The biomarker profile of ID largely consisted of pro-inflammatory markers, including paraoxonase 3 (PON3) and tartrate-resistant acid phosphatase type 5. In multivariable Cox proportional hazard regression analyses, ID was associated to worse outcome, independently of predictors of ID (hazard ratio 1.25, 95% confidence interval 1.06-1.46; P = 0.007).
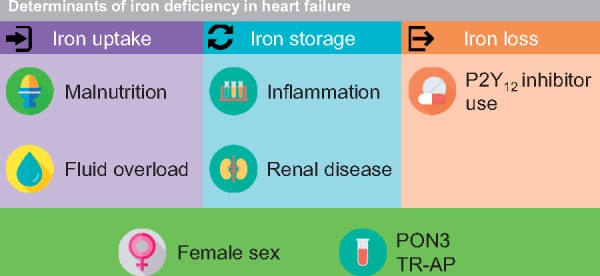
Conclusion: Our data suggest that the aetiology of ID in worsening HF is complex, multifactorial and seems to consist of a combination of reduced iron uptake (malnutrition, fluid overload), impaired iron storage (inflammation, chronic kidney disease), and iron loss (antiplatelets).
Keywords: Antiplatelets; Fluid retention; Heart failure; Inflammation; Iron deficiency; Protein intake.
© The Author(s) 2019. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Klip IT, Comin-Colet J, Voors AA, Ponikowski P, Enjuanes C, Banasiak W, Lok DJ, Rosentryt P, Torrens A, Polonski L, van Veldhuisen DJ, van der Meer P, Jankowska EA.. Iron deficiency in chronic heart failure: an international pooled analysis. Am Heart J 2013;165:575–582.e3. - PubMed
-
- van Veldhuisen DJ, Anker SD, Ponikowski P, Macdougall IC.. Anemia and iron deficiency in heart failure: mechanisms and therapeutic approaches. Nat Rev Cardiol 2011;8:485–493. - PubMed
-
- Jankowska EA, Rozentryt P, Witkowska A, Nowak J, Hartmann O, Ponikowska B, Borodulin-Nadzieja L, Banasiak W, Polonski L, Filippatos G, McMurray JJ, Anker SD, Ponikowski P.. Iron deficiency: an ominous sign in patients with systolic chronic heart failure. Eur Heart J 2010;31:1872–1880. - PubMed
-
- Okonko DO, Mandal AK, Missouris CG, Poole-Wilson PA.. Disordered iron homeostasis in chronic heart failure: prevalence, predictors, and relation to anemia, exercise capacity, and survival. J Am Coll Cardiol 2011;58:1241–1251. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
