

Neoadjuvant Modified FOLFOX6 With or Without Radiation Versus Fluorouracil Plus Radiation for Locally Advanced Rectal Cancer: Final Results of the Chinese FOWARC Trial
- PMID: 31557064
- PMCID: PMC6881102
- DOI: 10.1200/JCO.18.02309
Neoadjuvant Modified FOLFOX6 With or Without Radiation Versus Fluorouracil Plus Radiation for Locally Advanced Rectal Cancer: Final Results of the Chinese FOWARC Trial
Abstract
Purpose: In the multicenter, open-label, phase III FOWARC trial, modified infusional fluorouracil, leucovorin, and oxaliplatin (mFOLFOX6) plus radiotherapy resulted in a higher pathologic complete response rate than fluorouracil plus radiotherapy in Chinese patients with locally advanced rectal cancer. Here, we report the final results.
Methods: Adults ages 18 to 75 years with stage II/III rectal cancer were randomly assigned (1:1:1) to five cycles of infusional fluorouracil (leucovorin 400 mg/m2, fluorouracil 400 mg/m2, and fluorouracil 2.4 g/m2 over 48 hours) plus radiotherapy (46.0 to 50.4 Gy delivered in 23 to 25 fractions during cycles 2 to 4) followed by surgery and seven cycles of infusional fluorouracil, the same treatment plus intravenous oxaliplatin 85 mg/m2 on day 1 of each cycle (mFOLFOX6), or four to six cycles of mFOLFOX6 followed by surgery and six to eight cycles of mFOLFOX6. The primary end point was 3-year disease-free survival (DFS).
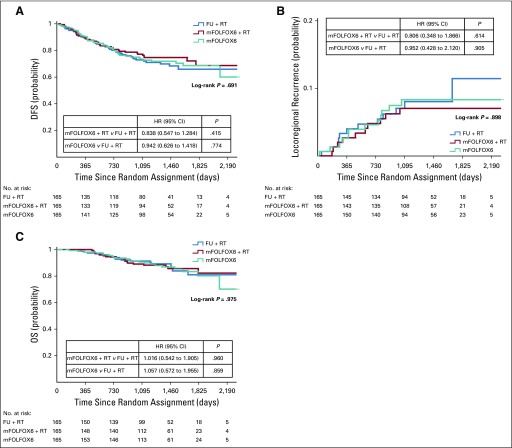
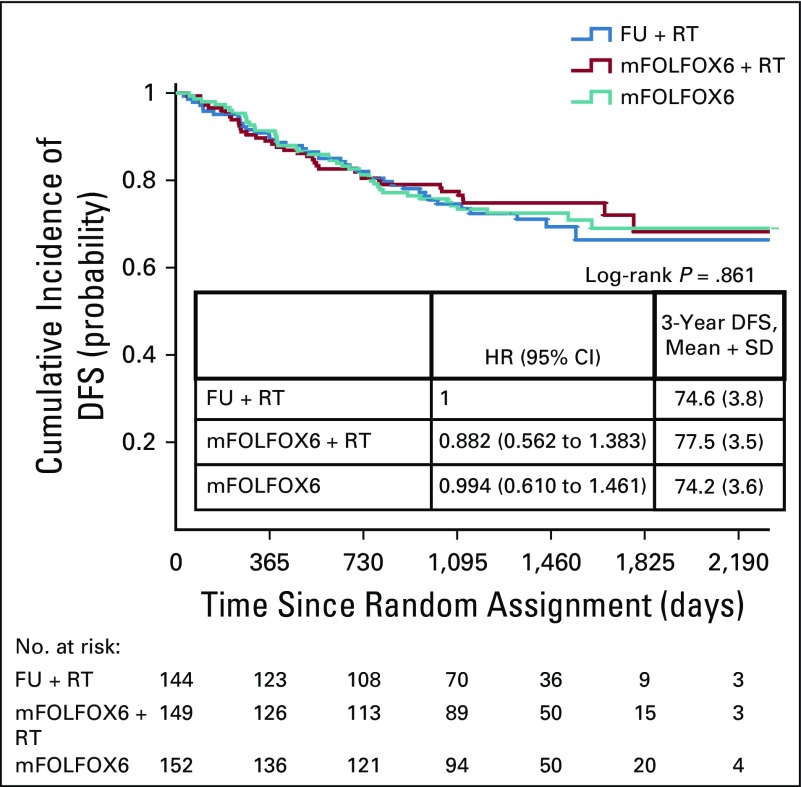
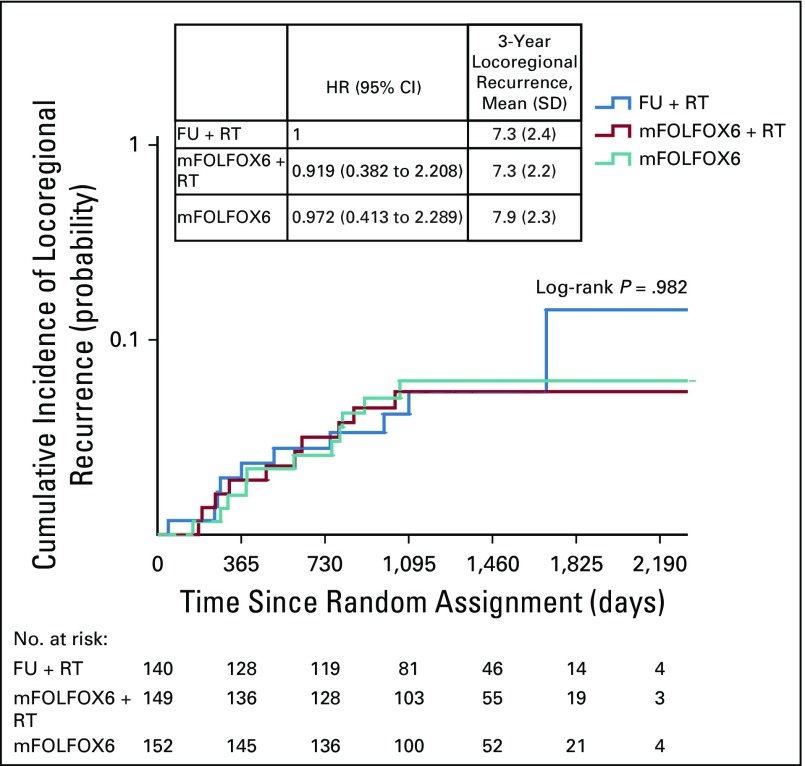
Results: In total, 495 patients were randomly assigned to treatment. After a median follow-up of 45.2 months, DFS events were reported in 46, 39, and 46 patients in the fluorouracil plus radiotherapy, mFOLFOX6 plus radiotherapy, and mFOLFOX6 arms. In each arm, the probability of 3-year DFS was 72.9%, 77.2%, and 73.5% (P = .709 by the log-rank test), the 3-year probability of local recurrence after R0/1 resection was 8.0%, 7.0%, and 8.3% (P = .873 by the log-rank test), and the 3-year overall survival rate was 91.3%, 89.1%, and 90.7% (P = .971 by log-rank test), respectively.
Conclusion: mFOLFOX6, with or without radiation, did not significantly improve 3-year DFS versus fluorouracil with radiation in patients with locally advanced rectal cancer. No significant difference in outcomes was found between mFOLFOX6 without radiotherapy and fluorouracil with radiotherapy, which requires additional investigation of the role of radiotherapy in these regimens.
Trial registration: ClinicalTrials.gov NCT01211210.
Figures


References
-
- Gérard JP, Conroy T, Bonnetain F, et al. Preoperative radiotherapy with or without concurrent fluorouracil and leucovorin in T3-4 rectal cancers: Results of FFCD 9203. J Clin Oncol. 2006;24:4620–4625. - PubMed
-
- Rahbari NN, Elbers H, Askoxylakis V, et al. Neoadjuvant radiotherapy for rectal cancer: Meta-analysis of randomized controlled trials. Ann Surg Oncol. 2013;20:4169–4182. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
LinkOut - more resources
Full Text Sources
Medical
