

Analyzing data from the digital healthcare exchange platform for surveillance of antibiotic prescriptions in primary care in urban Kenya: A mixed-methods study
- PMID: 31557170
- PMCID: PMC6762089
- DOI: 10.1371/journal.pone.0222651
Analyzing data from the digital healthcare exchange platform for surveillance of antibiotic prescriptions in primary care in urban Kenya: A mixed-methods study
Erratum in
-
Correction: Analyzing data from the digital healthcare exchange platform for surveillance of antibiotic prescriptions in primary care in urban Kenya: A mixed-methods study.PLoS One. 2019 Nov 21;14(11):e0225846. doi: 10.1371/journal.pone.0225846. eCollection 2019. PLoS One. 2019. PMID: 31751418 Free PMC article.
Abstract
Background: Knowledge of antibiotic prescription practices in low- and middle-income countries is limited due to a lack of adequate surveillance systems.
Objective: To assess the prescription of antibiotics for the treatment of acute respiratory tract infections (ARIs) in primary care.
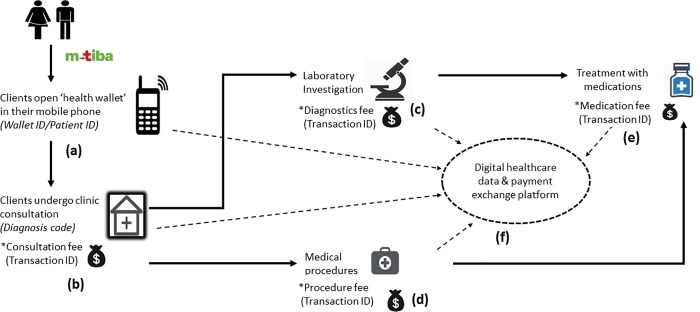
Method: An explanatory sequential mixed-methods study was conducted in 4 private not-for-profit outreach clinics located in slum areas in Nairobi, Kenya. Claims data of patients who received healthcare between April 1 and December 27, 2016 were collected in real-time through a mobile telephone-based healthcare data and payment exchange platform (branded as M-TIBA). These data were used to calculate the percentage of ARIs for which antibiotics were prescribed. In-depth interviews were conducted among 12 clinicians and 17 patients to explain the quantitative results.
Results: A total of 49,098 individuals were registered onto the platform, which allowed them to access healthcare at the study clinics through M-TIBA. For 36,210 clinic visits by 21,913 patients, 45,706 diagnoses and 85,484 medication prescriptions were recorded. ARIs were the most common diagnoses (17,739; 38.8%), and antibiotics were the most frequently prescribed medications (21,870; 25.6%). For 78.5% (95% CI: 77.9%, 79.1%) of ARI diagnoses, antibiotics were prescribed, most commonly amoxicillin (45%; 95% CI: 44.1%, 45.8%). These relatively high levels of prescription were explained by high patient load, clinician and patient perceptions that clinicians should prescribe, lack of access to laboratory tests, offloading near-expiry drugs, absence of policy and surveillance, and the use of treatment guidelines that are not up-to-date. Clinicians in contrast reported to strictly follow the Kenyan treatment guidelines.
Conclusion: This study showed successful quantification of antibiotic prescription and the prescribing pattern using real-world data collected through M-TIBA in private not-for-profit clinics in Nairobi.
Conflict of interest statement
AIGHD received funding from Joep Lange Institute to conduct this research. M-TIBA is rolled out by CarePay Ltd, Kenya. No authors declare a conflict of interest. Neither Joep Lange Institute nor CarePay had a role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. We confirm our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- WHO. Antimicrobial Resistance. Accessed on Aug 1, 2017 at: http://www.who.int/antimicrobial-resistance/en/
-
- U.S. Department of Health and Human Services, Centers for disease control and Prevention [USA]. Antibiotic resistance threats in the United States, 2013. Accessed on October 10, 2017 at: https://www.cdc.gov/drugresistance/threat-report-2013/pdf/ar-threats-201...
-
- Center for Disease Dynamics, Economics & Policy. 2015. State of the World’s Antibiotics, 2015. CDDEP: Washington, D.C., USA.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
