

Deep-learning model for predicting 30-day postoperative mortality
- PMID: 31558311
- PMCID: PMC6993109
- DOI: 10.1016/j.bja.2019.07.025
Deep-learning model for predicting 30-day postoperative mortality
Abstract
Background: Postoperative mortality occurs in 1-2% of patients undergoing major inpatient surgery. The currently available prediction tools using summaries of intraoperative data are limited by their inability to reflect shifting risk associated with intraoperative physiological perturbations. We sought to compare similar benchmarks to a deep-learning algorithm predicting postoperative 30-day mortality.
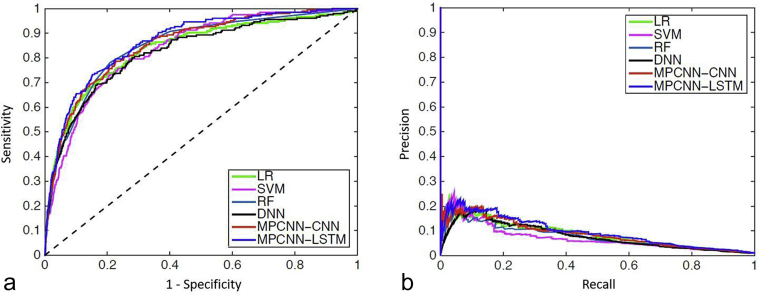
Methods: We constructed a multipath convolutional neural network model using patient characteristics, co-morbid conditions, preoperative laboratory values, and intraoperative numerical data from patients undergoing surgery with tracheal intubation at a single medical centre. Data for 60 min prior to a randomly selected time point were utilised. Model performance was compared with a deep neural network, a random forest, a support vector machine, and a logistic regression using predetermined summary statistics of intraoperative data.
Results: Of 95 907 patients, 941 (1%) died within 30 days. The multipath convolutional neural network predicted postoperative 30-day mortality with an area under the receiver operating characteristic curve of 0.867 (95% confidence interval [CI]: 0.835-0.899). This was higher than that for the deep neural network (0.825; 95% CI: 0.790-0.860), random forest (0.848; 95% CI: 0.815-0.882), support vector machine (0.836; 95% CI: 0.802-870), and logistic regression (0.837; 95% CI: 0.803-0.871).
Conclusions: A deep-learning time-series model improves prediction compared with models with simple summaries of intraoperative data. We have created a model that can be used in real time to detect dynamic changes in a patient's risk for postoperative mortality.
Keywords: anaesthesiology; deep learning; machine learning; postoperative complications; risk prediction; surgery.
Copyright © 2019 British Journal of Anaesthesia. Published by Elsevier Ltd. All rights reserved.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures


Comment in
-
Deep learning for risk assessment: all about automatic feature extraction.Br J Anaesth. 2020 Feb;124(2):131-133. doi: 10.1016/j.bja.2019.10.017. Epub 2019 Dec 6. Br J Anaesth. 2020. PMID: 31813571 No abstract available.
-
Update to 'Deep-learning model for predicting 30-day postoperative mortality' (Br J Anaesth 2019; 123: 688-95).Br J Anaesth. 2020 Aug;125(2):e230-e231. doi: 10.1016/j.bja.2020.04.010. Epub 2020 May 7. Br J Anaesth. 2020. PMID: 32389391 Free PMC article. No abstract available.
References
-
- GlobalSurg Collaborative Mortality of emergency abdominal surgery in high-, middle-, and low-income countries. Br J Surg. 2016;103:971–988. - PubMed
-
- Moonesinghe S.R., Mythen M.G., Das P., Rowan K.M., Grocott M.P.W. Risk stratification tools for predicting morbidity and mortality in adult patients undergoing major surgery: qualitative systematic review. Anesthesiology. 2013;119:959–981. - PubMed
-
- Dawson N.V., Arkes H.R. Systematic errors in medical decision making: judgement limitations. J Gen Intern Med. 1987;2:183–187. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
