

Pre- and Postoperative Neratinib for HER2-Positive Breast Cancer Brain Metastases: Translational Breast Cancer Research Consortium 022
- PMID: 31558424
- PMCID: PMC7035200
- DOI: 10.1016/j.clbc.2019.07.011
Pre- and Postoperative Neratinib for HER2-Positive Breast Cancer Brain Metastases: Translational Breast Cancer Research Consortium 022
Abstract
Purpose: This pilot study was performed to test our ability to administer neratinib monotherapy before clinically recommended craniotomy in patients with HER2-positive metastatic breast cancer to the central nervous system, to examine neratinib's central nervous system penetration at craniotomy, and to examine postoperative neratinib maintenance.
Patients and methods: Patients with HER2-positive brain metastases undergoing clinically indicated cranial resection of a parenchymal tumor received neratinib 240 mg orally once a day for 7 to 21 days preoperatively, and resumed therapy postoperatively in 28-day cycles. Exploratory evaluations of time to disease progression, survival, and correlative tissue, cerebrospinal fluid (CSF), and blood-based analyses examining neratinib concentrations were planned. The study was registered at ClinicalTrials.gov under number NCT01494662.
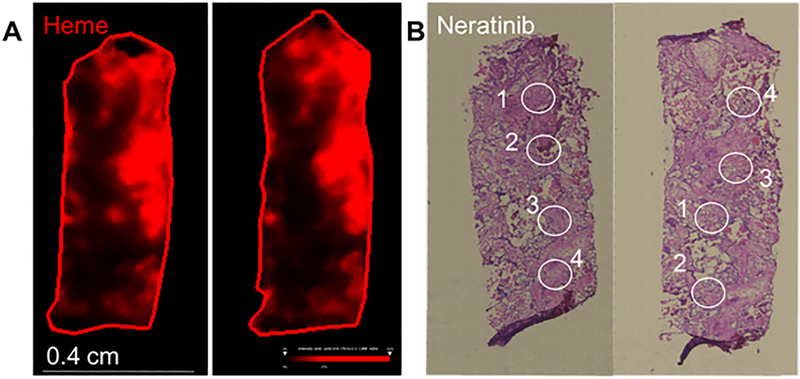
Results: We enrolled 5 patients between May 22, 2013, and October 18, 2016. As of March 1, 2019, patients had remained on the study protocol for 1 to 75+ postoperative cycles pf therapy. Two patients had grade 3 diarrhea. Evaluation of the CSF showed low concentrations of neratinib; nonetheless, 2 patients continued to receive therapy without disease progression for at least 13 cycles, with one on-study treatment lasting for nearly 6 years. Neratinib distribution in surgical tissue was variable for 1 patient, while specimens from 2 others did not produce conclusive results as a result of limited available samples.
Conclusion: Neratinib resulted in expected rates of diarrhea in this small cohort, with 2 of 5 patients receiving the study treatment for durable periods. Although logistically challenging, we were able to test a limited number of CSF- and parenchymal-based neratinib concentrations. Our findings from resected tumor tissue in one patient revealed heterogeneity in drug distribution and tumor histopathology.
Keywords: Central nervous system; Metastatic.
Copyright © 2019 Elsevier Inc. All rights reserved.
Figures
References
-
- Lin NU, Winer EP. Brain metastases: the HER2 paradigm. Clin Cancer Res. 2007;13(6):1648–1655. - PubMed
-
- Bendell JC, Domchek SM, Burstein HJ, et al. Central nervous system metastases in women who receive trastuzumab-based therapy for metastatic breast carcinoma. Cancer. 2003;97(12):2972–2977. - PubMed
-
- Lin NU, Bellon JR, Winer EP. CNS metastases in breast cancer. J Clin Oncol. 2004;22(17):3608–3617. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
