

Unintended Consequences of mHealth Interactive Voice Messages Promoting Contraceptive Use After Menstrual Regulation in Bangladesh: Intimate Partner Violence Results From a Randomized Controlled Trial
- PMID: 31558596
- PMCID: PMC6816818
- DOI: 10.9745/GHSP-D-19-00015
Unintended Consequences of mHealth Interactive Voice Messages Promoting Contraceptive Use After Menstrual Regulation in Bangladesh: Intimate Partner Violence Results From a Randomized Controlled Trial
Abstract
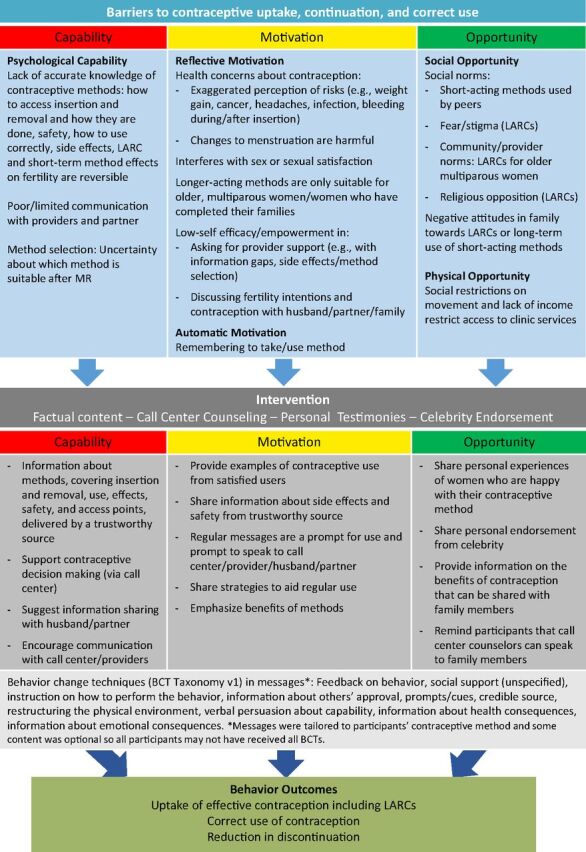
Background: Mobile phones for health (mHealth) hold promise for delivering behavioral interventions. We evaluated the effect of automated interactive voice messages promoting contraceptive use with a focus on long-acting reversible contraceptives (LARCs) among women in Bangladesh who had undergone menstrual regulation (MR), a procedure to "regulate the menstrual cycle when menstruation is absent for a short duration."
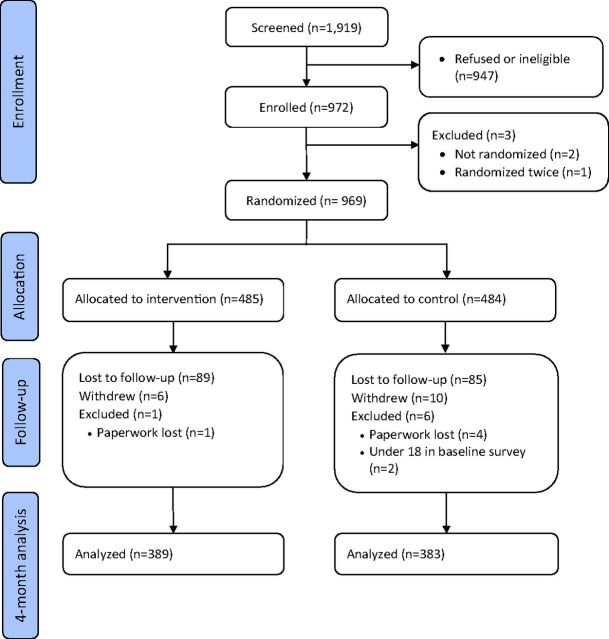
Methods: We recruited MR clients from 41 public- and private-sector clinics immediately after MR. Eligibility criteria included having a personal mobile phone and consenting to receive messages about family planning by phone. We randomized participants remotely to an intervention group that received at least 11 voice messages about contraception over 4 months or to a control group (no messages). The primary outcome was LARC use at 4 months. Adverse events measured included experience of intimate partner violence (IPV). Researchers recruiting participants and 1 analyst were blinded to allocation groups. All analyses were intention to treat. The trial is registered with ClinicalTrials.gov (NCT02579785).
Results: Between December 2015 and March 2016, 485 women were allocated to the intervention group and 484 to the control group. We completed follow-up on 389 intervention and 383 control participants. Forty-eight (12%) participants in the intervention group and 59 (15%) in the control group reported using a LARC method at 4 months (adjusted odds ratio [aOR] using multiple imputation=0.95; 95% confidence interval [CI]=0.49 to 1.83; P=.22). Reported physical IPV was higher in the intervention group: 42 (11%) intervention versus 25 (7%) control (aOR=1.97; 95% CI=1.12 to 3.46; P=.03) when measured using a closed question naming acts of violence. No violence was reported in response to an open question about effects of being in the study.
Conclusions: The intervention did not increase LARC use but had an unintended consequence of increasing self-reported IPV. Researchers and health program designers should consider possible negative impacts when designing and evaluating mHealth and other reproductive health interventions. IPV must be measured using closed questions naming acts of violence.
© Reiss et al.
Figures
References
-
- National Institute of Population Research and Training (NIPORT), Mitra and Associates, ICF International. Bangladesh Demographic and Health Survey 2014. Dhaka, Bangladesh and Rockville, MD: NIPORT, Mitra and Associates, ICF International; 2016. http://dhsprogram.com/pubs/pdf/FR311/FR311.pdf. Accessed June 21, 2016.
-
- Sonfield A, Hasstedt K, Kavanaugh ML, Anderson R. The Social and Economic Benefits of Women's Ability to Determine Whether and When to Have Children. New York, NY: Guttmacher Institute; 2013. https://www.guttmacher.org/sites/default/files/report_pdf/social-economi.... Accessed June 21, 2019.
-
- World Health Organization Department of Reproductive Health and Research (WHO/RHR), Johns Hopkins Bloomberg School of Public Health/Center for Communication Programs (CCP), Knowledge for Health Project. Family Planning: A Global Handbook for Providers (2018 Update). Baltimore, MD, and Geneva, Switzerland: CCP and WHO; 2018. http://apps.who.int/iris/bitstream/handle/10665/260156/9780999203705-eng.... Accessed June 21, 2019.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical