

MUC5B variant is associated with visually and quantitatively detected preclinical pulmonary fibrosis
- PMID: 31558622
- PMCID: PMC7535073
- DOI: 10.1136/thoraxjnl-2018-212430
MUC5B variant is associated with visually and quantitatively detected preclinical pulmonary fibrosis
Abstract
Background: Relatives of patients with familial interstitial pneumonia (FIP) are at increased risk for pulmonary fibrosis. We assessed the prevalence and risk factors for preclinical pulmonary fibrosis (PrePF) in first-degree relatives of patients with FIP and determined the utility of deep learning in detecting PrePF on CT.
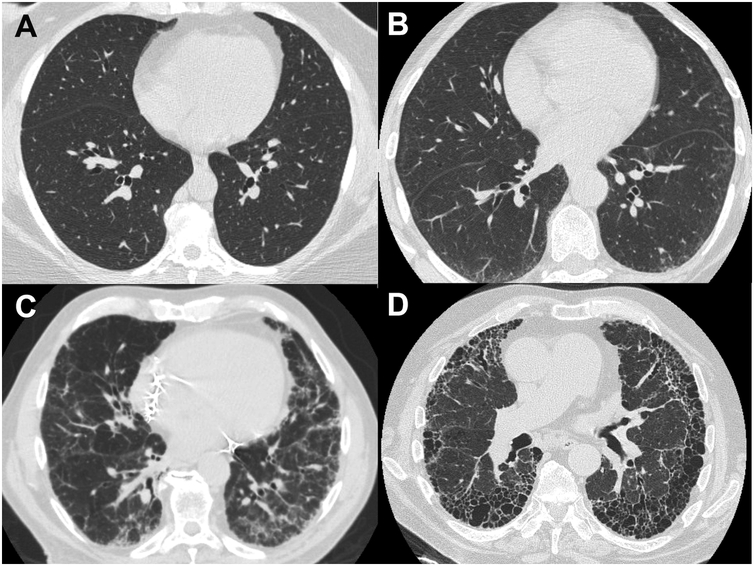
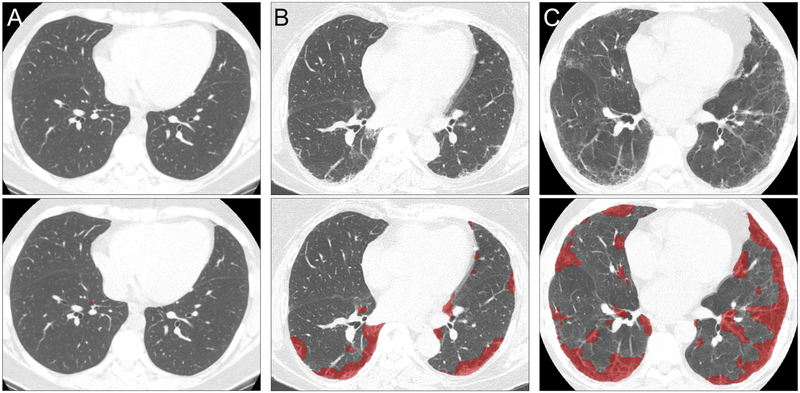
Methods: First-degree relatives of patients with FIP over 40 years of age who believed themselves to be unaffected by pulmonary fibrosis underwent CT scans of the chest. Images were visually reviewed, and a deep learning algorithm was used to quantify lung fibrosis. Genotyping for common idiopathic pulmonary fibrosis risk variants in MUC5B and TERT was performed.
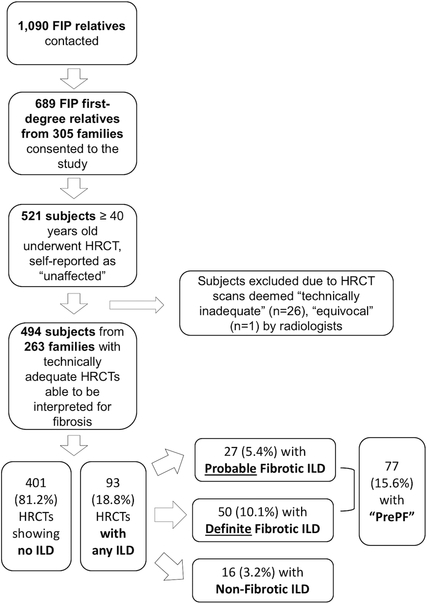
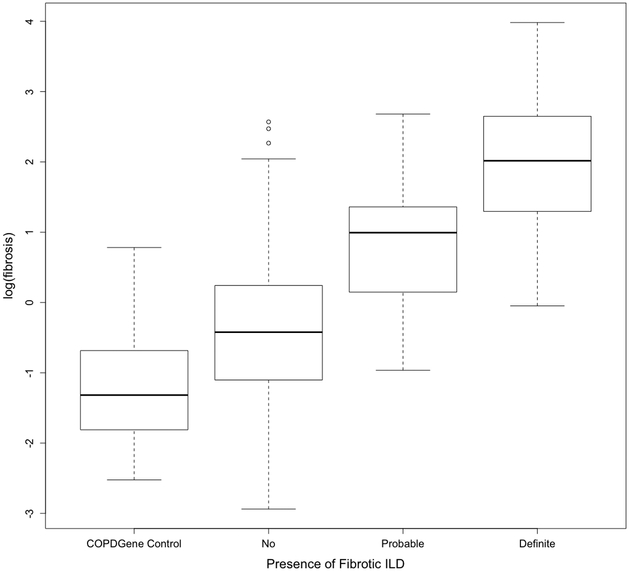
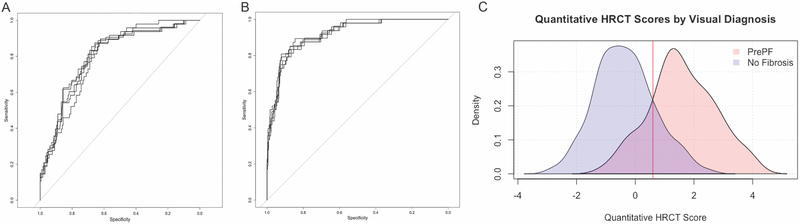
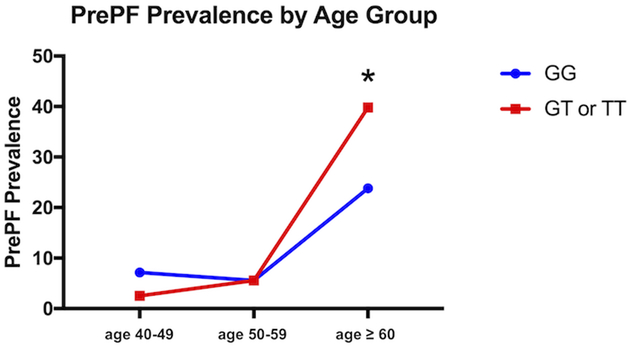
Findings: In 494 relatives of patients with FIP from 263 families of patients with FIP, the prevalence of PrePF on visual CT evaluation was 15.6% (95% CI 12.6 to 19.0). Compared with visual CT evaluation, deep learning quantitative CT analysis had 84% sensitivity (95% CI 0.72 to 0.89) and 86% sensitivity (95% CI 0.83 to 0.89) for discriminating subjects with visual PrePF diagnosis. Subjects with PrePF were older (65.9, SD 10.1 years) than subjects without fibrosis (55.8 SD 8.7 years), more likely to be male (49% vs 37%), more likely to have smoked (44% vs 27%) and more likely to have the MUC5B promoter variant rs35705950 (minor allele frequency 0.29 vs 0.21). MUC5B variant carriers had higher quantitative CT fibrosis scores (mean difference of 0.36%), a difference that remains significant when controlling for age and sex.
Interpretation: PrePF is common in relatives of patients with FIP. Its prevalence increases with age and the presence of a common MUC5B promoter variant. Quantitative CT analysis can detect these imaging abnormalities.
Keywords: Idiopathic pulmonary fibrosis; Imaging/CT MRI etc; Interstitial Fibrosis.
© Author(s) (or their employer(s)) 2019. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: DAS is the founder and chief scientific officer of Eleven P15, a company focused on the early diagnosis and treatment of pulmonary fibrosis. DAS has an awarded patent (US patent no: 8,673,565) for the treatment and diagnosis of fibrotic lung disease. DAL and SMH have a pending patent (application US20170330320A1) for image analysis; SMH reports a consulting agreement with Boehringer Ingelheim.
Figures
Comment in
-
MUC5B promoter variant: genomic fingerprint for early identification of undiagnosed pulmonary fibrosis.Thorax. 2019 Dec;74(12):1111-1112. doi: 10.1136/thoraxjnl-2019-214061. Epub 2019 Oct 30. Thorax. 2019. PMID: 31666387 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources