

Autologous haematopoietic stem cell transplantation and other cellular therapy in multiple sclerosis and immune-mediated neurological diseases: updated guidelines and recommendations from the EBMT Autoimmune Diseases Working Party (ADWP) and the Joint Accreditation Committee of EBMT and ISCT (JACIE)
- PMID: 31558790
- PMCID: PMC6995781
- DOI: 10.1038/s41409-019-0684-0
Autologous haematopoietic stem cell transplantation and other cellular therapy in multiple sclerosis and immune-mediated neurological diseases: updated guidelines and recommendations from the EBMT Autoimmune Diseases Working Party (ADWP) and the Joint Accreditation Committee of EBMT and ISCT (JACIE)
Abstract
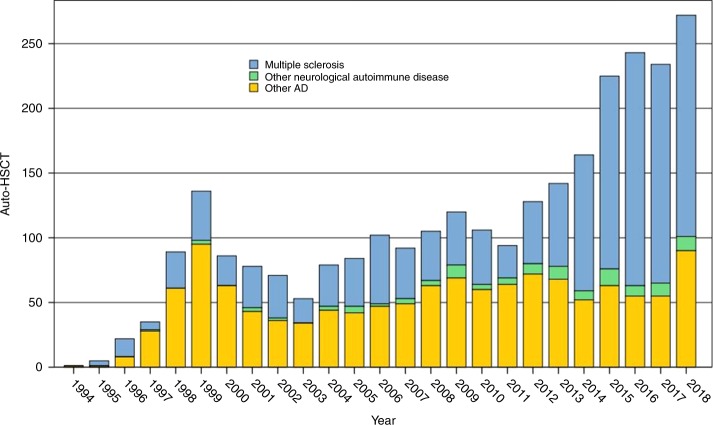
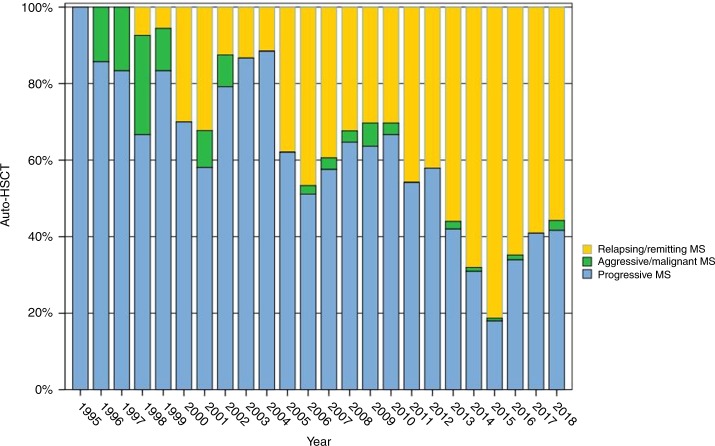
These updated EBMT guidelines review the clinical evidence, registry activity and mechanisms of action of haematopoietic stem cell transplantation (HSCT) in multiple sclerosis (MS) and other immune-mediated neurological diseases and provide recommendations for patient selection, transplant technique, follow-up and future development. The major focus is on autologous HSCT (aHSCT), used in MS for over two decades and currently the fastest growing indication for this treatment in Europe, with increasing evidence to support its use in highly active relapsing remitting MS failing to respond to disease modifying therapies. aHSCT may have a potential role in the treatment of the progressive forms of MS with a significant inflammatory component and other immune-mediated neurological diseases, including chronic inflammatory demyelinating polyneuropathy, neuromyelitis optica, myasthenia gravis and stiff person syndrome. Allogeneic HSCT should only be considered where potential risks are justified. Compared with other immunomodulatory treatments, HSCT is associated with greater short-term risks and requires close interspeciality collaboration between transplant physicians and neurologists with a special interest in these neurological conditions before, during and after treatment in accredited HSCT centres. Other experimental cell therapies are developmental for these diseases and patients should only be treated on clinical trials.
Conflict of interest statement
JAS declares speaker fees at educational events supported by Sanofi, Janssen, Jazz, Mallinckrodt and Gilead, is a member of a trial IDMC for Kiadis Pharma and Chairs NHS England Clinical Reference Group (CRG) for Blood and Marrow Transplantation. RM has received personal remuneration for advisory functions and presentations by Merck, Teva, Sanofi, Novartis, Roche, Biogen, Cell Protect and Neuway Pharma. He is a co-founder and co-owner of Cellerys. PAM reports personal fees and non-financial support from Bayer, Biogen, Merck and Novartis, unrelated to the manuscript. PAM, BS and JS are grateful for support from the UK NIHR EME and Biomedical Research Centre funding schemes. The other authors declare no competing interests.
Figures


References
-
- Moccia M, Palladino R, Lanzillo R, Carotenuto A, Russo C, Triassi M, et al. Healthcare costs for treating relapsing multiple sclerosis and the risk of progression: a retrospective Italian cohort study from 2001 to 2015. PLoS One. 2017;12:e0169489. doi: 10.1371/journal.pone.0169489. - DOI - PMC - PubMed
