

Multidisciplinary approach in the management of uterine intravenous leiomyomatosis with intracardiac extension: case report and review of literature
- PMID: 31558962
- PMCID: PMC6738492
- DOI: 10.3941/jrcr.v13i7.3607
Multidisciplinary approach in the management of uterine intravenous leiomyomatosis with intracardiac extension: case report and review of literature
Abstract
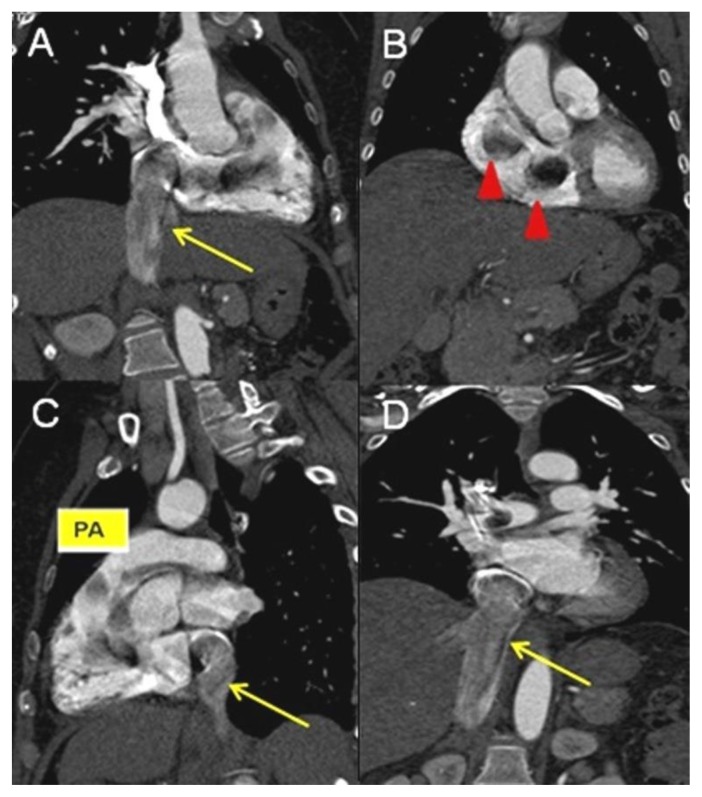
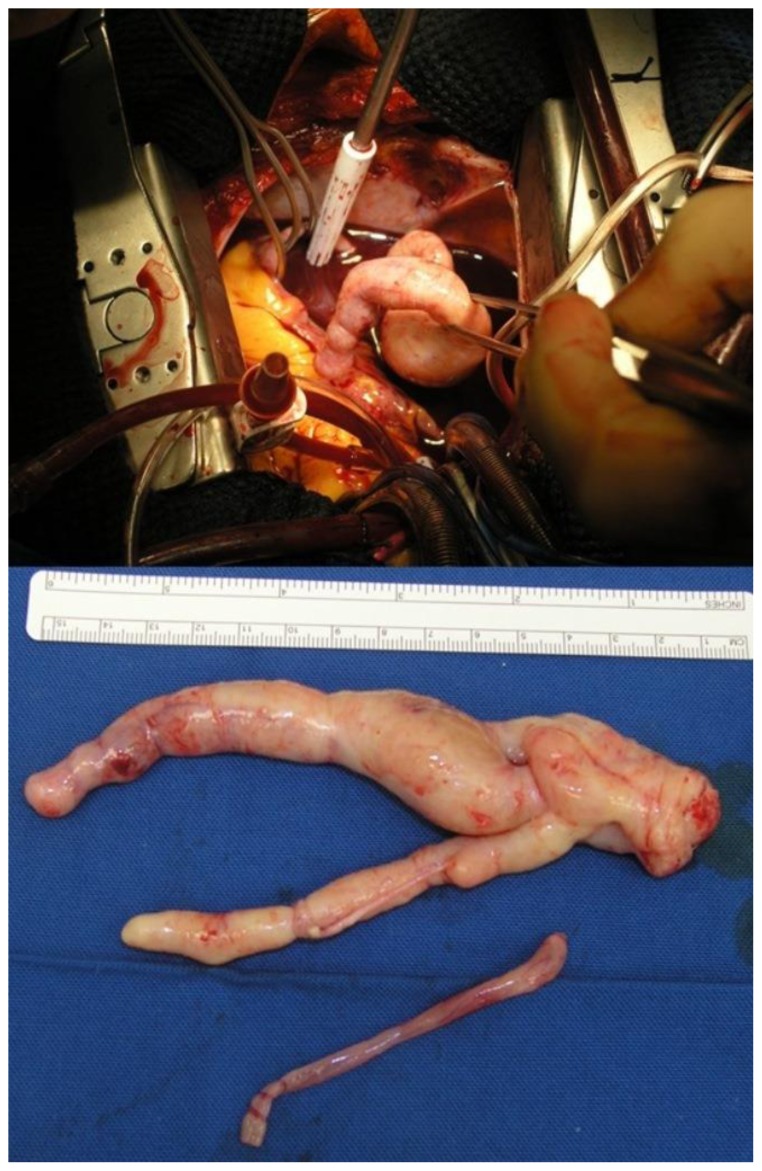
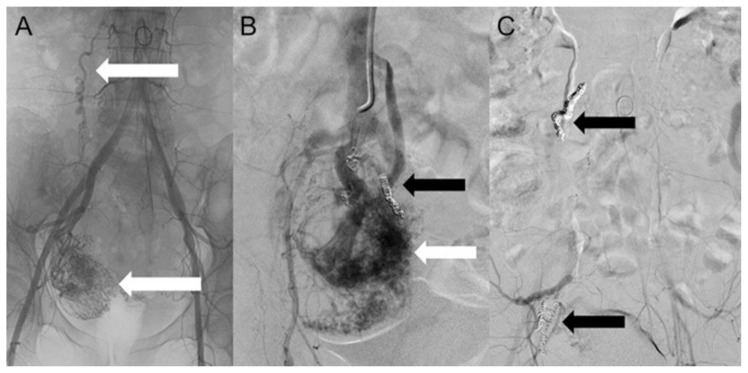
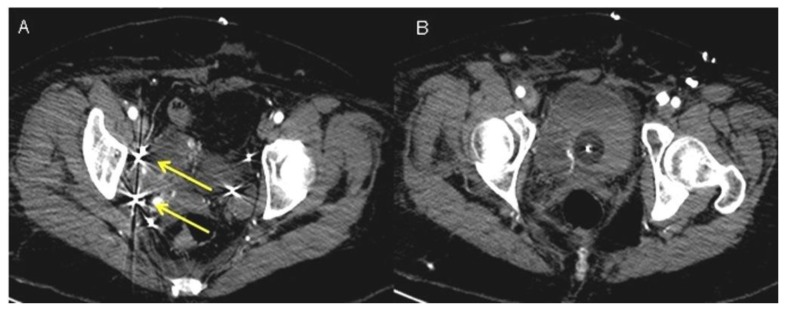
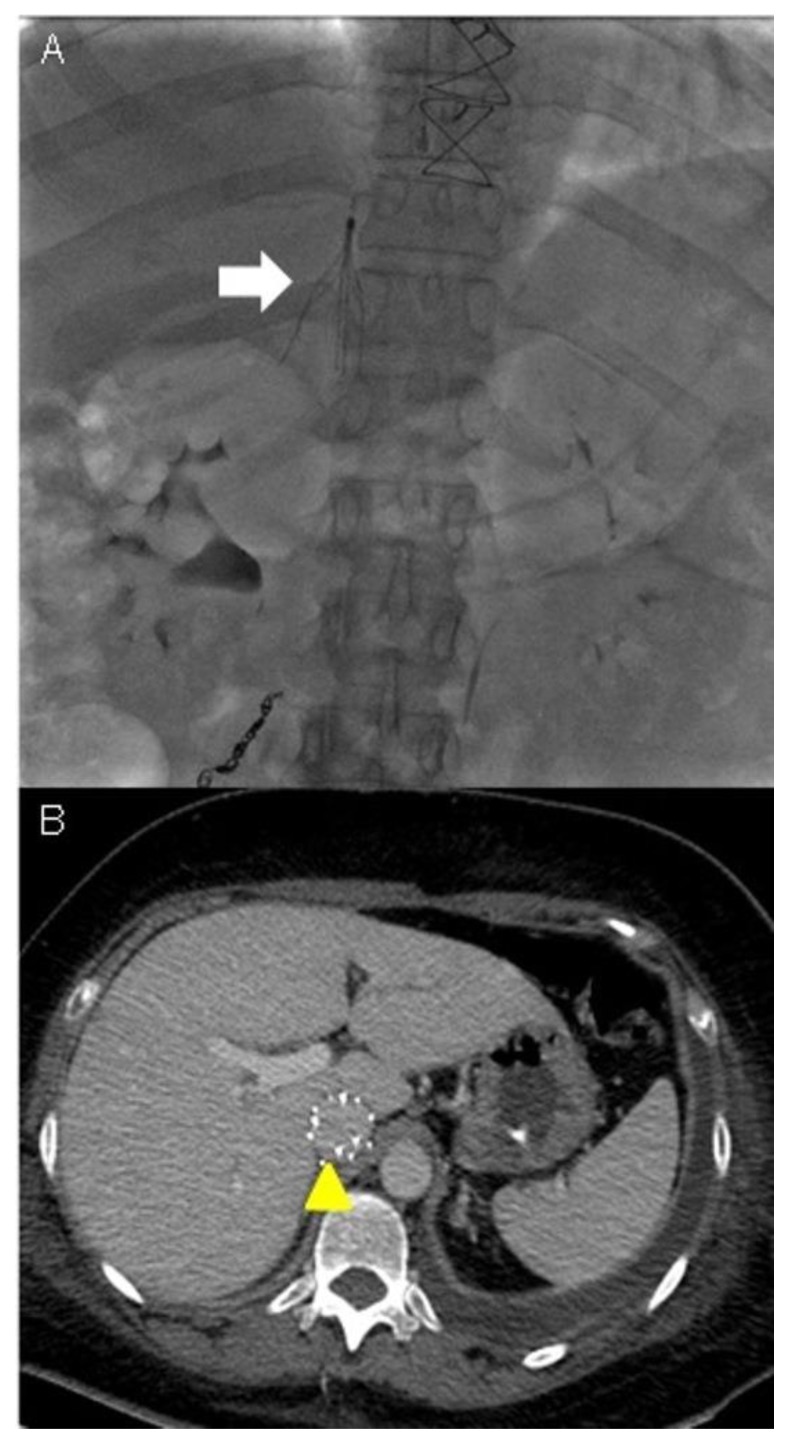
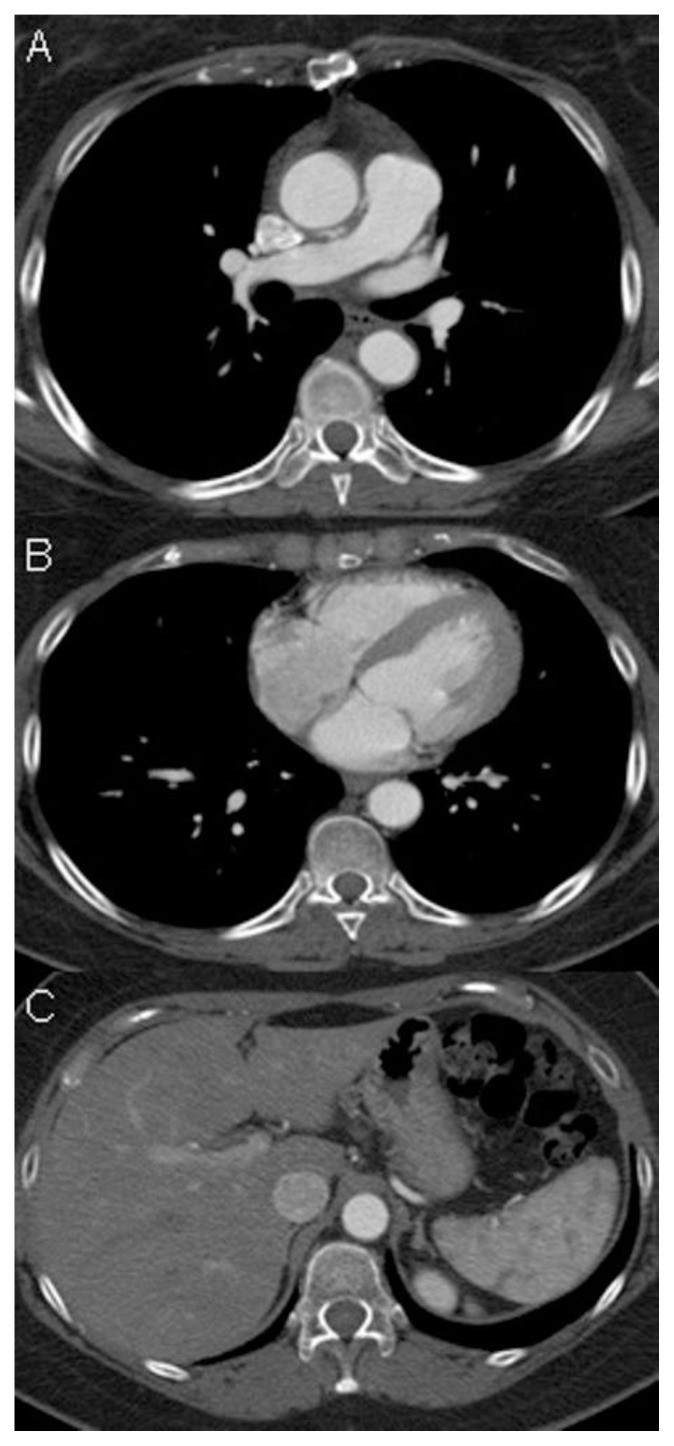
Uterine intravenous leiomyomatosis is an uncommon tumor, usually arising from the uterus, with nodular masses which extend intravascularly over variable distances and may reach the inferior vena cava, right atrium, and pulmonary arteries. Early diagnosis and surgical intervention are crucial as intracardiac leiomyomatosis not only causes cardiac symptoms but may result in pulmonary embolism and sudden death. Complete tumor resection is key in disease management, thus rendering cardiac-extending uterine intravenous leiomyomatosis one of the most challenging conditions for surgical treatment. The use of interventional radiology procedures can facilitate the surgical approach. We report the case of a massive pelvic recurrence of uterine leiomyomatosis with intracardiac extension and pulmonary embolism, analyzing management and surgical outcomes, highlighting the role of interventional radiology during the therapeutic pathway. Nonetheless, there are currently very few data available concerning the use of interventional radiology procedures in the therapeutic strategy of uterine intravenous leiomyomatosis with intracardiac extension.
Keywords: Computed Tomography angiography; Percutaneous embolizazion; Uterine intravenous leiomyomatosis; inferior vena cava filter; intracardiac extension.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical