

A retrospective study analyzing missed diagnosis of lung metastases at their early stages on computed tomography
- PMID: 31559039
- PMCID: PMC6753459
- DOI: 10.21037/jtd.2019.08.19
A retrospective study analyzing missed diagnosis of lung metastases at their early stages on computed tomography
Abstract
Background: Lungs are one of the target organs of metastases of primary lung, breast, liver, colorectal, and esophageal cancer. While computed tomography (CT) is the most widely used modality for detecting lung metastases, it is still very challenging to detect them at the earlier stages. If lung metastases could be found on CT scans at the earliest time points, patients would benefit by beginning treatment earlier. The objective of this study was to demonstrate that CT can reveal lung metastases in many cases at even earlier stages than current radiological practice may find.
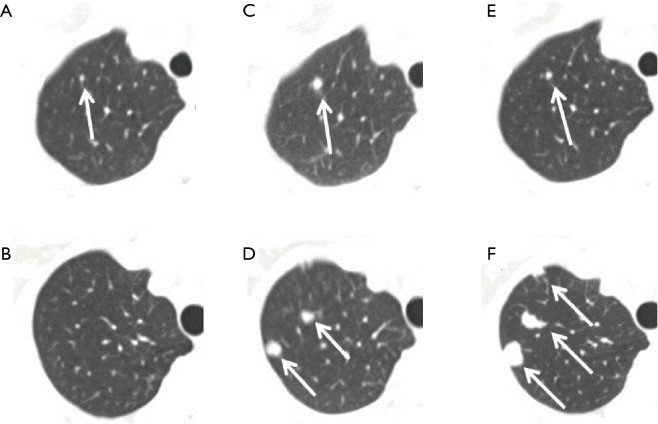
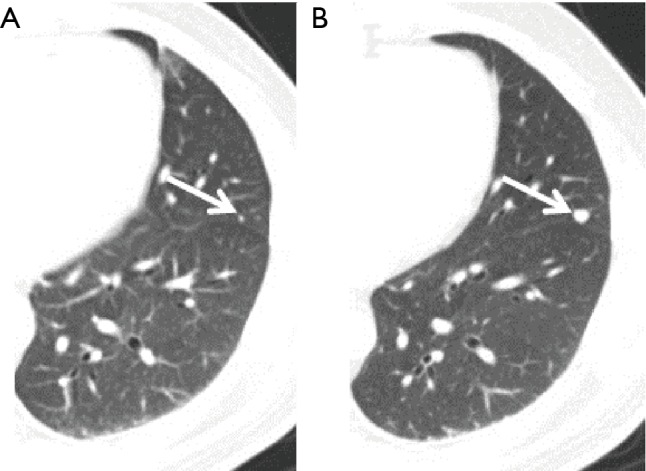
Methods: One hundred patients with lung metastases were randomly selected and their surveillance CT scans were analyzed retrospectively. The patients had primary cancer in the breasts, lungs, esophagus, colorectum, and liver. All patients had multiple CT examinations of the lungs and their metastases, if any, were confirmed by subsequent CT scans. The earliest CT scans were examined to determine whether lung metastases at the same locations had been diagnosed or missed. Missed lung metastases, categorized by type of the primary cancer and adjacency to nearby blood vessels, were statistically analyzed.
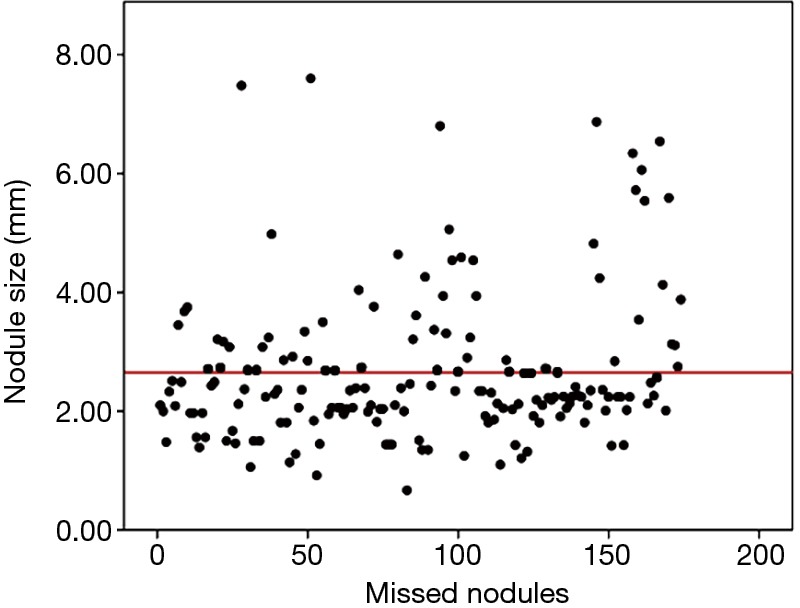
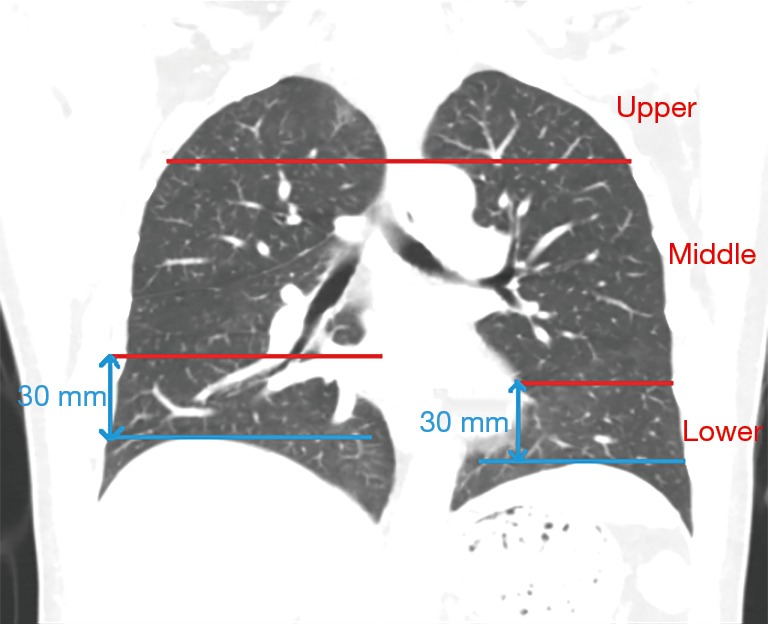
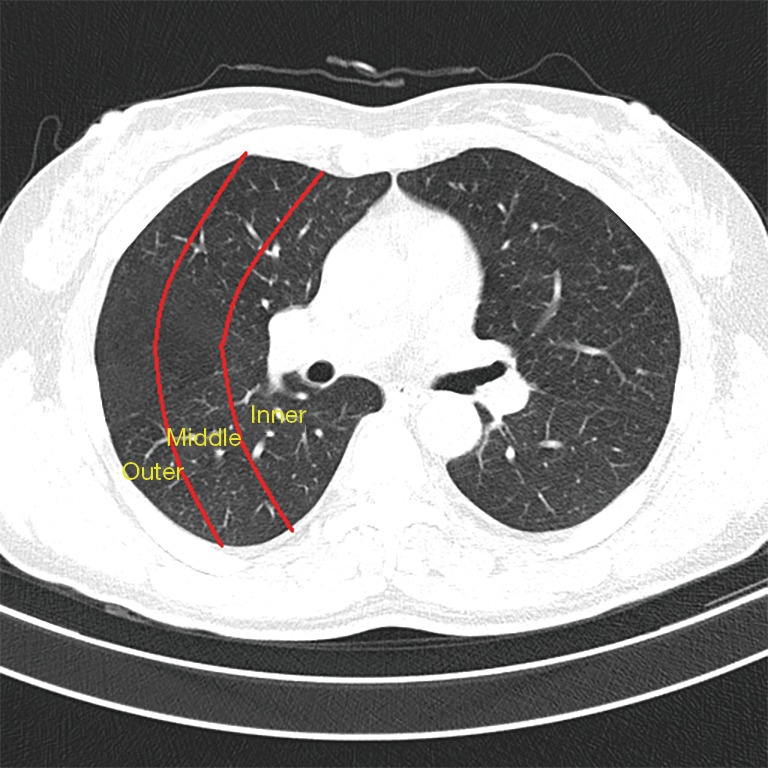
Results: There were 36/100 (36%) cases of missed lung metastases, including 15 cases of single metastasis and 21 cases of multiple metastases. There were a total of 174 missed loci of lung metastases. Where metastases were missed, there was a statistically significant difference (P<0.001) in their distribution within the sub-regions of the lungs. Adjacency to blood vessels appeared to be a significant factor in metastases being missed during diagnosis (P<0.001).
Conclusions: There was a considerable percentage of early lung metastases that were missed by radiologists but actually appeared on CT scans. The capability of CT to reveal such early metastases opens up an opportunity to move up the time points of detecting lung metastases through clinical and training improvement and technology development such as computer-aided detection.
Keywords: Computed tomography (CT); early detection; lung metastases.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources