

Pulmonary arteries: imaging of pulmonary embolism and beyond
- PMID: 31559153
- PMCID: PMC6732114
- DOI: 10.21037/cdt.2018.08.05
Pulmonary arteries: imaging of pulmonary embolism and beyond
Abstract
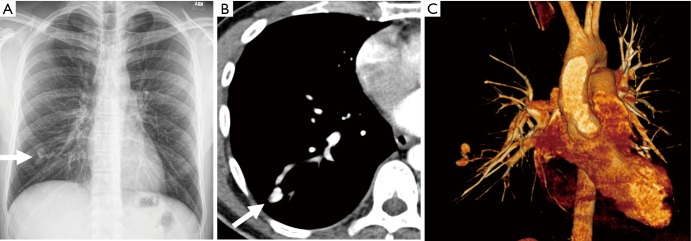
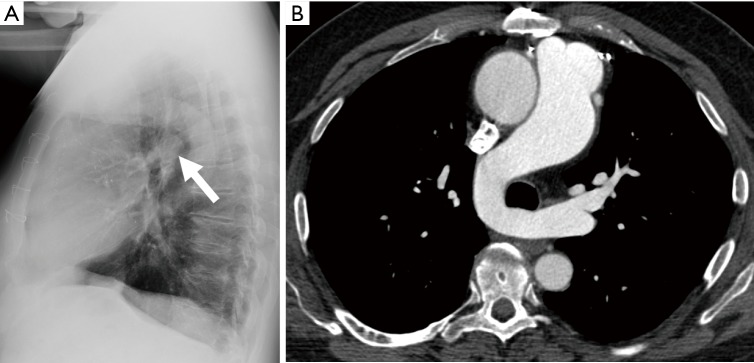
The pulmonary arteries are not just affected by thrombus. Various acquired and congenital conditions can also affect the pulmonary arteries. In this review we discuss cross sectional imaging modalities utilized for the imaging of the pulmonary arteries. Acquired pulmonary artery entities, including pulmonary artery sarcoma (PAS), vasculitis, aneurysm, and arteriovenous malformations, and congenital anomalies in adults, including proximal interruption of the pulmonary artery, pulmonary sling, pulmonary artery stenosis, and idiopathic dilatation of the pulmonary trunk, are also discussed. An awareness of these entities and their imaging findings is important for radiologists interpreting chest imaging.
Keywords: Computed tomography (CT); congenital anomalies; pulmonary arteriovenous malformation; pulmonary artery aneurysm; pulmonary artery sarcoma (PAS); pulmonary embolus (PE).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources