

Vascular imaging in renal donors
- PMID: 31559158
- PMCID: PMC6732115
- DOI: 10.21037/cdt.2018.11.02
Vascular imaging in renal donors
Abstract
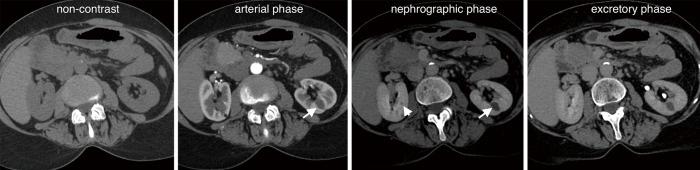
Imaging plays a crucial role in pre-transplant evaluation to enhance the probability of a successful outcome. Its aim is to define kidney and vascular anatomy and to assess potential pathologies. Each modality has advantages and disadvantages. Computed tomography angiography (CTA) is the most commonly used imaging modality, however, magnetic resonance angiography (MRA) can be used in selected cases. The purpose of this review article is to provide an overview of available imaging modalities, their benefits, risks, advantages, and disadvantages. Imaging findings that indicate particular anomalies and pathologies that may affect living renal donor selection will be discussed.
Keywords: Renal donor; transplantation; vascular imaging.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
















References
Publication types
LinkOut - more resources
Full Text Sources