

Portal-Mesenteric Vein Resection in Borderline Pancreatic Cancer; 33 Month-Survival in Patients with Good Performance Status
- PMID: 31559380
- PMCID: PMC6761582
- DOI: 10.1089/pancan.2019.0013
Portal-Mesenteric Vein Resection in Borderline Pancreatic Cancer; 33 Month-Survival in Patients with Good Performance Status
Abstract
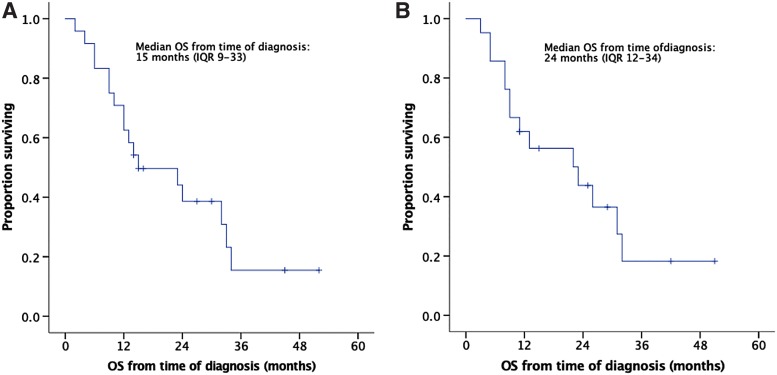
Background: Patients with pancreatic cancer (PC), which is not upfront resectable, but borderline, involving major peripancreatic vessels, have not been generally considered for surgery, considering that resection in such a setting may be futile. Materials and Methods: Retrospective analysis of prospectively collected data on patients with borderline pancreatic adenocarcinoma undergoing pancreatectomy en-block with portal and/or superior mesenteric vein resection in a tertiary referral center in Greece between January 2012 and February 2017. Follow-up was complete up to January 2018. Results: Twenty-four patients were included. Neoadjuvant therapy (NAT) was administered to only 38%, but more commonly in the second half of the group (58% vs. 17%, p = 0.035). It was associated with smaller tumor size (median: 2.5 vs. 4.2 cm, p < 0.001), fewer positive lymph nodes (LNs) in the resected specimen (median: 2 vs. 5, p = 0.04), and higher likelihood of adjuvant therapy (78% vs. 40%, p = 0.01), but not with survival. Resection was extensive: a median of 26 LNs were retrieved, R0 resection rate (≥1 mm) was 79%, and median length of vein segments was 4 cm, requiring interposition grafts in 58% (mostly polytetrafluoroethylene). Median intensive care unit stay was 0 days and length of hospital stay was 9 days. Post-operative mortality was 12.5%. Median overall survival was 24 months. Eastern Cooperative Oncology Group (ECOG) status was significantly associated with survival (p < 0.001) with ECOG-0: 33 months, ECOG-1: 12 months, and ECOG-2: 6 months. Conclusion: This first Greek national series of portomesenteric vein resection in borderline PC demonstrates that it results to 2 years of median survival, extending to 33 months in patients with good performance status, especially if NAT is uniformly administered.
Keywords: borderline pancreatic cancer; locally advanced pancreatic cancer; mesenteric vein resection; pancreaticoduodenectomy; portal vein resection.
Conflict of interest statement
No competing financial interests exist.
Figures


References
-
- Tsiotos GG, Farnell MB, Sarr MG. Are the results of pancreatectomy for pancreatic cancer really improving? World J Surg. 1999;23:913–919 - PubMed
-
- Nigri G, Petrucciani N, Pinna AD, et al. . Evolution of pancreatectomy with en bloc venous resection for pancreatic cancer in Italy. Retrospective cohort study of 425 cases in 10 pancreatic referral units. Int J Surg. 2018;55:103–109 - PubMed
-
- Michelakos T, Pergolini I, Castillo CF, et al. . Predictors of resectability and survival in patients with borderline and locally advanced pancreatic cancer who underwent neoadjuvant treatment with FOLFIRINOX. Ann Surg. 2019;269:733–740 - PubMed
-
- Hackert T, Sachsenmeier M, Hinz U, et al. . Locally advanced pancreatic cancer: neoadjuvant therapy with folfirinox results in resectability in 60% of the patients. Ann Surg. 2016;264:457–463 - PubMed
LinkOut - more resources
Full Text Sources
Research Materials