

Emergence of the Asian lineage of Zika virus in Angola: an outbreak investigation
- PMID: 31559967
- PMCID: PMC6892302
- DOI: 10.1016/S1473-3099(19)30293-2
Emergence of the Asian lineage of Zika virus in Angola: an outbreak investigation
Abstract
Background: Zika virus infections and suspected microcephaly cases have been reported in Angola since late 2016, but no data are available about the origins, epidemiology, and diversity of the virus. We aimed to investigate the emergence and circulation of Zika virus in Angola.
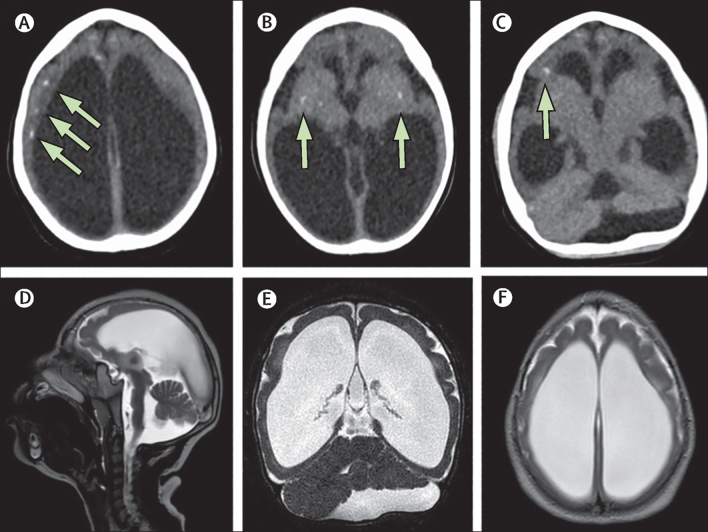
Methods: Diagnostic samples collected by the Angolan Ministry of Health as part of routine arboviral surveillance were tested by real-time reverse transcription PCR by the Instituto Nacional de Investigação em Saúde (Ministry of Health, Luanda, Angola). To identify further samples positive for Zika virus and appropriate for genomic sequencing, we also tested samples from a 2017 study of people with HIV in Luanda. Portable sequencing was used to generate Angolan Zika virus genome sequences from three people positive for Zika virus infection by real-time reverse transcription PCR, including one neonate with microcephaly. Genetic and mobility data were analysed to investigate the date of introduction and geographical origin of Zika virus in Angola. Brain CT and MRI, and serological assays were done on a child with microcephaly to confirm microcephaly and assess previous Zika virus infection.
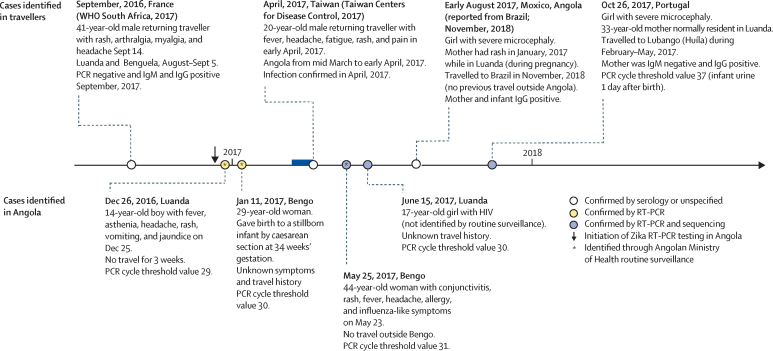
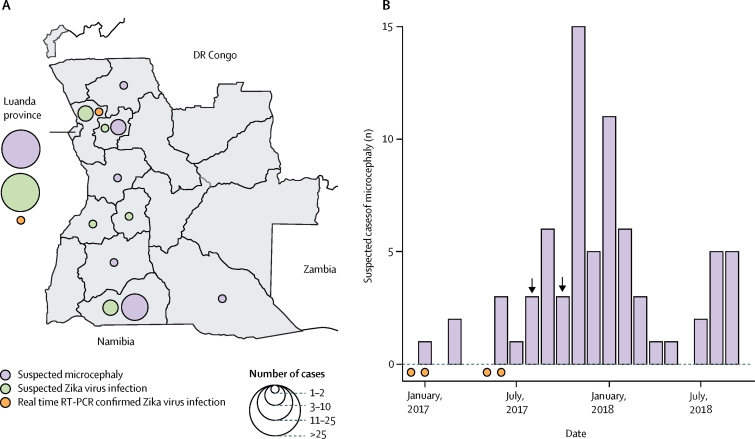
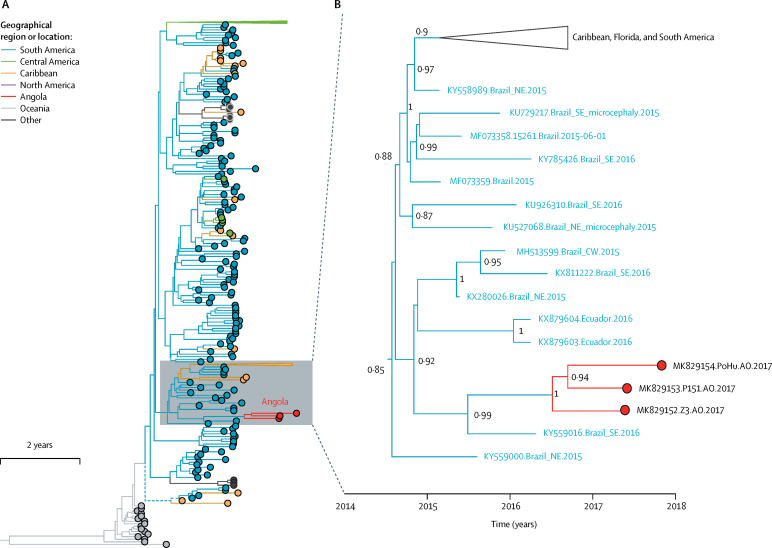
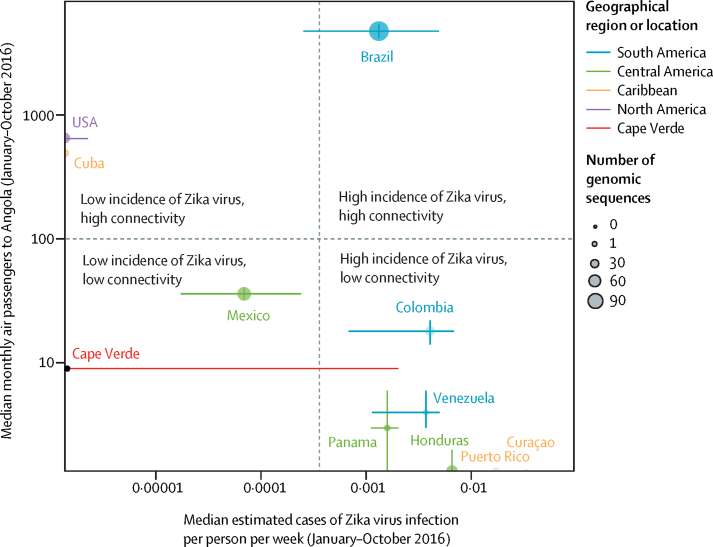
Findings: Serum samples from 54 people with suspected acute Zika virus infection, 76 infants with suspected microcephaly, 24 mothers of infants with suspected microcephaly, 336 patients with suspected dengue virus or chikungunya virus infection, and 349 samples from the HIV study were tested by real-time reverse transcription PCR. Four cases identified between December, 2016, and June, 2017, tested positive for Zika virus. Analyses of viral genomic and human mobility data suggest that Zika virus was probably introduced to Angola from Brazil between July, 2015, and June, 2016. This introduction probably initiated local circulation of Zika virus in Angola that continued until at least June, 2017. The infant with microcephaly in whom CT and MRI were done had brain abnormalities consistent with congenital Zika syndrome and serological evidence for Zika virus infection.
Interpretation: Our analyses show that autochthonous transmission of the Asian lineage of Zika virus has taken place in Africa. Zika virus surveillance and surveillance of associated cases of microcephaly throughout the continent is crucial.
Funding: Royal Society, Wellcome Trust, Global Challenges Research Fund (UK Research and Innovation), Africa Oxford, John Fell Fund, Oxford Martin School, European Research Council, Departamento de Ciência e Tecnologia/Ministério da Saúde/National Council for Scientific and Technological Development, and Ministério da Educação/Coordenação de Aperfeicoamento de Pessoal de Nível Superior.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Better surveillance to protect mothers and infants from Zika.Lancet Infect Dis. 2019 Oct;19(10):1047-1048. doi: 10.1016/S1473-3099(19)30473-6. Lancet Infect Dis. 2019. PMID: 31559951 Free PMC article. No abstract available.
-
Long-term surveillance needed to detect Zika virus outbreaks in endemic regions.Lancet Infect Dis. 2020 Feb;20(2):168-169. doi: 10.1016/S1473-3099(19)30677-2. Lancet Infect Dis. 2020. PMID: 32006504 No abstract available.
References
-
- Baud D, Gubler DJ, Schaub B, Lanteri MC, Musso D. An update on Zika virus infection. Lancet. 2017;390:2099–2109. - PubMed
-
- Pan American Health Organization. WHO Zika cases and congenital syndrome associated with Zika virus reported by countries and territories in the Americas, 2015–2018 cumulative cases. 2018. https://www.paho.org/hq/index.php?option=com_docman&view=download&catego...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
