

Circulatory factors associated with function and prognosis in patients with severe heart failure
- PMID: 31562542
- PMCID: PMC7239817
- DOI: 10.1007/s00392-019-01554-3
Circulatory factors associated with function and prognosis in patients with severe heart failure
Abstract
Background: Multiple circulatory factors are increased in heart failure (HF). Many have been linked to cardiac and/or skeletal muscle tissue processes, which in turn might influence physical activity and/or capacity during HF. This study aimed to provide a better understanding of the mechanisms linking HF with the loss of peripheral function.
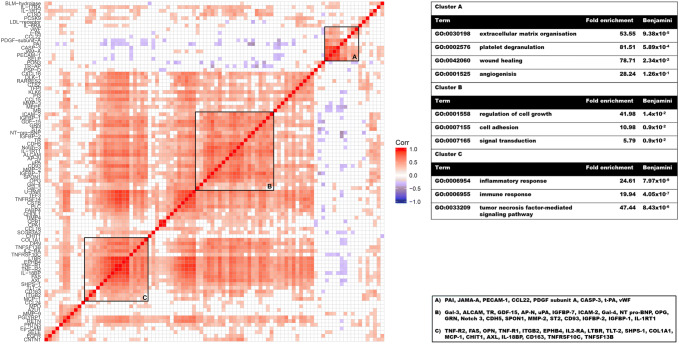
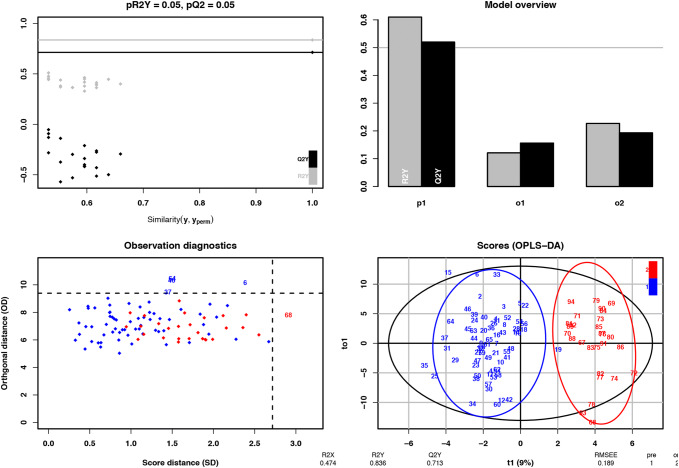
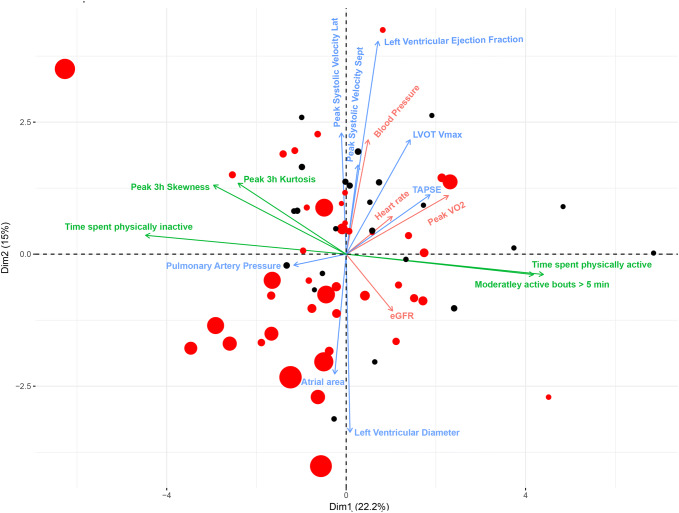
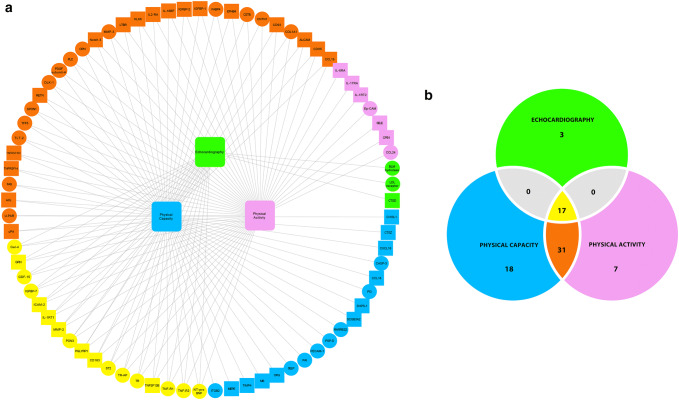
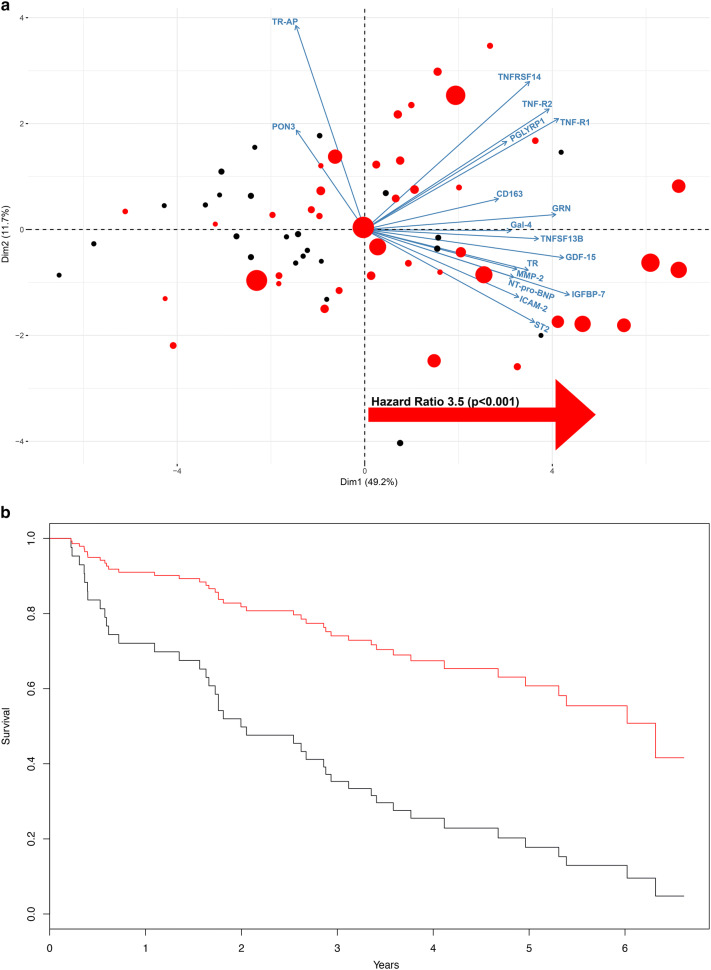
Methods and results: Physical capacity measured by maximum oxygen uptake, myocardial function (measured by echocardiography), physical activity (measured by accelerometry), and mortality data was collected for patients with severe symptomatic heart failure an ejection fraction < 35% (n = 66) and controls (n = 28). Plasma circulatory factors were quantified using a multiplex immunoassay. Multivariate (orthogonal projections to latent structures discriminant analysis) and univariate analyses identified many factors that differed significantly between HF and control subjects, mainly involving biological functions related to cell growth and cell adhesion, extracellular matrix organization, angiogenesis, and inflammation. Then, using principal component analysis, links between circulatory factors and physical capacity, daily physical activity, and myocardial function were identified. A subset of ten biomarkers differentially expressed in patients with HF vs controls covaried with physical capacity, daily physical activity, and myocardial function; eight of these also carried prognostic value. These included established plasma biomarkers of HF, such as NT-proBNP and ST2 along with recently identified factors such as GDF15, IGFBP7, and TfR, as well as a new factor, galectin-4.
Conclusions: These findings reinforce the importance of systemic circulatory factors linked to hemodynamic stress responses and inflammation in the pathogenesis and progress of HF disease. They also support established biomarkers for HF and suggest new plausible markers.
Keywords: Multiplex immunoassay; New york heart association (NYHA) functional classification; Orthogonal projections to latent structures discriminant analysis (OPLS-DA); Principal component analysis (PCA).
Conflict of interest statement
The authors declare that there are no conflicts of interest.
Figures
References
-
- Ahmad T, Fiuzat M, Neely B, Neely ML, Pencina MJ, Kraus WE, Zannad F, Whellan DJ, Donahue MP, Pina IL, Adams KF, Kitzman DW, O'Connor CM, Felker GM. Biomarkers of myocardial stress and fibrosis as predictors of mode of death in patients with chronic heart failure. JACC Heart Failure. 2014;2:260–268. doi: 10.1016/j.jchf.2013.12.004. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
