

A mathematical model of coagulation under flow identifies factor V as a modifier of thrombin generation in hemophilia A
- PMID: 31562694
- PMCID: PMC6994344
- DOI: 10.1111/jth.14653
A mathematical model of coagulation under flow identifies factor V as a modifier of thrombin generation in hemophilia A
Abstract
Background: The variability in bleeding patterns among individuals with hemophilia A, who have similar factor VIII (FVIII) levels, is significant and the origins are unknown.
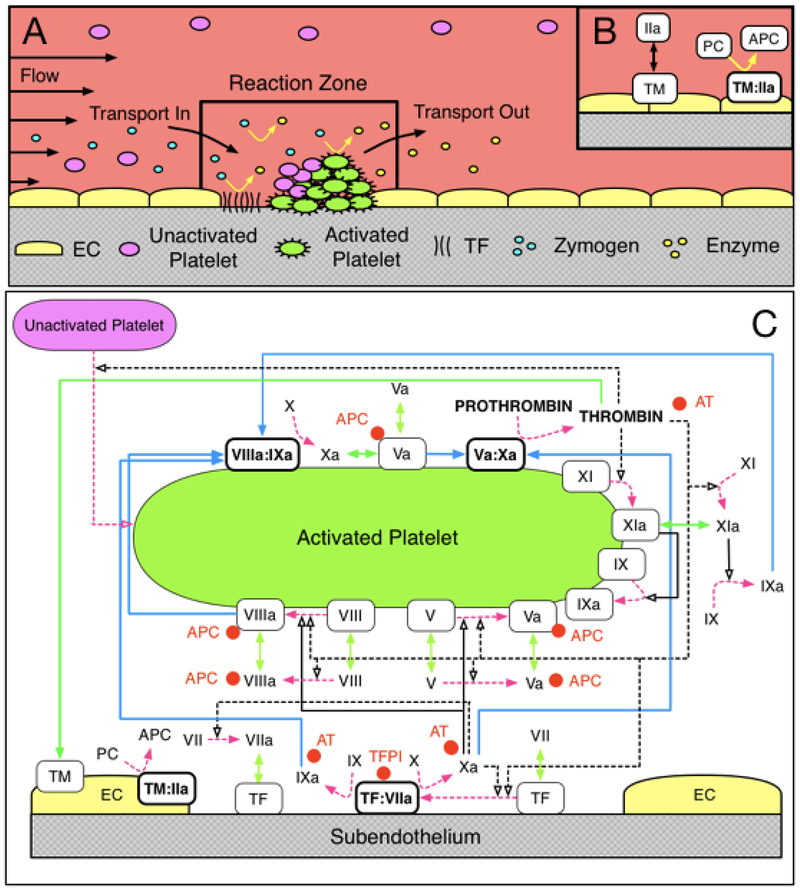
Objective: To use a previously validated mathematical model of flow-mediated coagulation as a screening tool to identify parameters that are most likely to enhance thrombin generation in the context of FVIII deficiency.
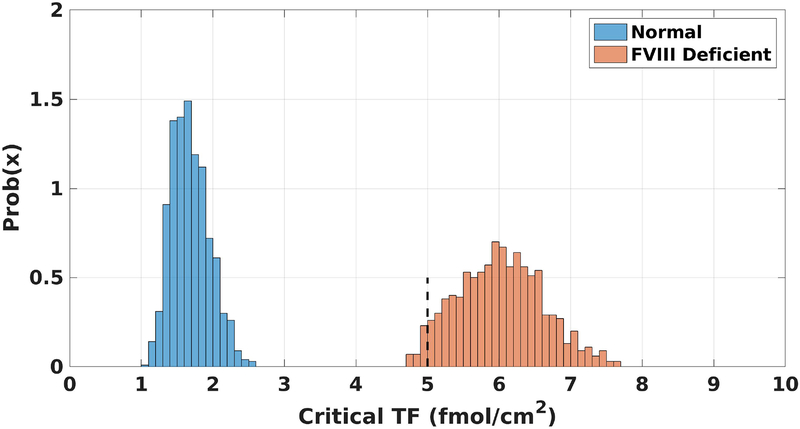
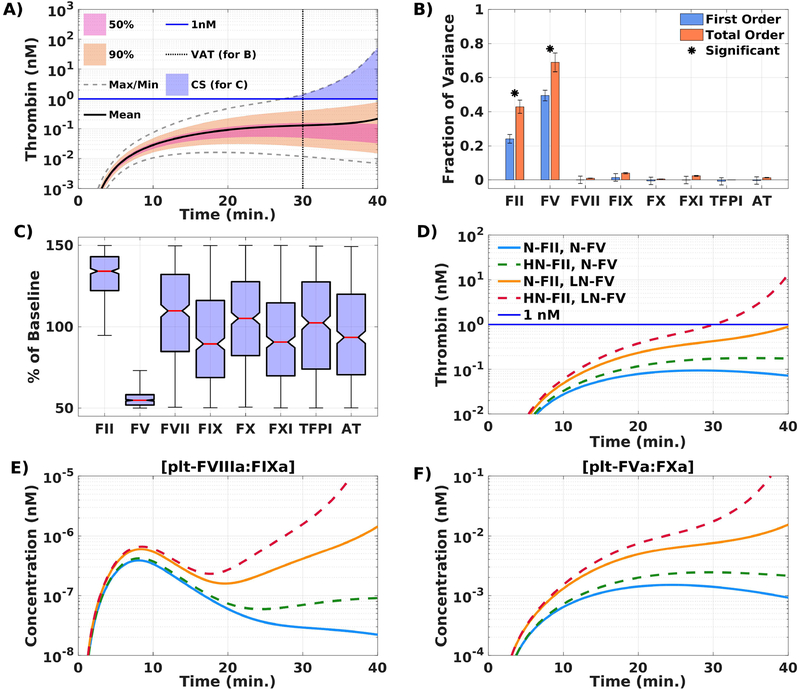
Methods: We performed a global sensitivity analysis (GSA) on our mathematical model to identify potential modifiers of thrombin generation. Candidates from the GSA were confirmed by calibrated automated thrombography (CAT) and flow assays on collagen-tissue factor (TF) surfaces at a shear rate of 100 per second.
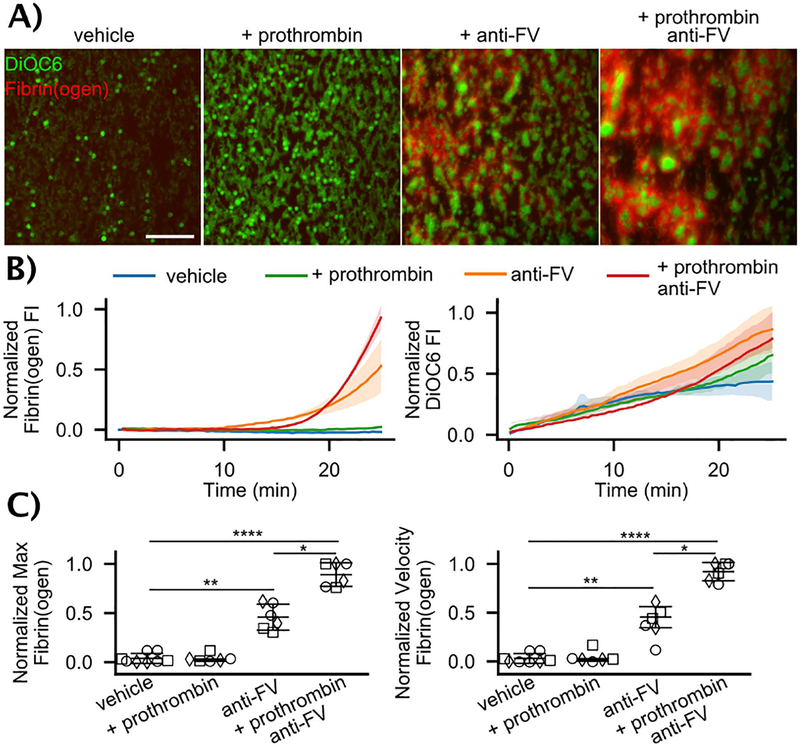
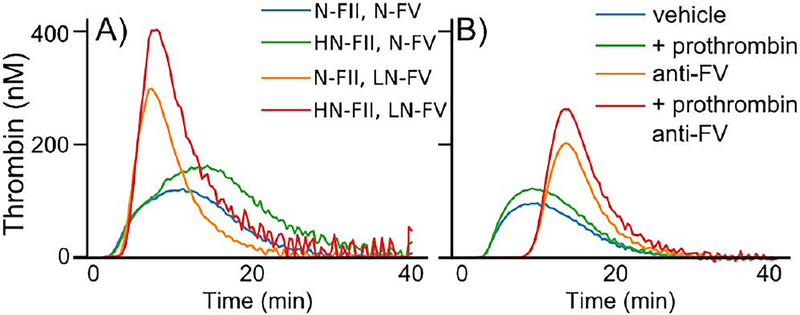
Results: Simulations identified low-normal factor V (FV) (50%) as the strongest modifier, with additional thrombin enhancement when combined with high-normal prothrombin (150%). Low-normal FV levels or partial FV inhibition (60% activity) augmented thrombin generation in FVIII-inhibited or FVIII-deficient plasma in CAT. Partial FV inhibition (60%) boosted fibrin deposition in flow assays performed with whole blood from individuals with mild and moderate FVIII deficiencies. These effects were amplified by high-normal prothrombin levels in both experimental models.
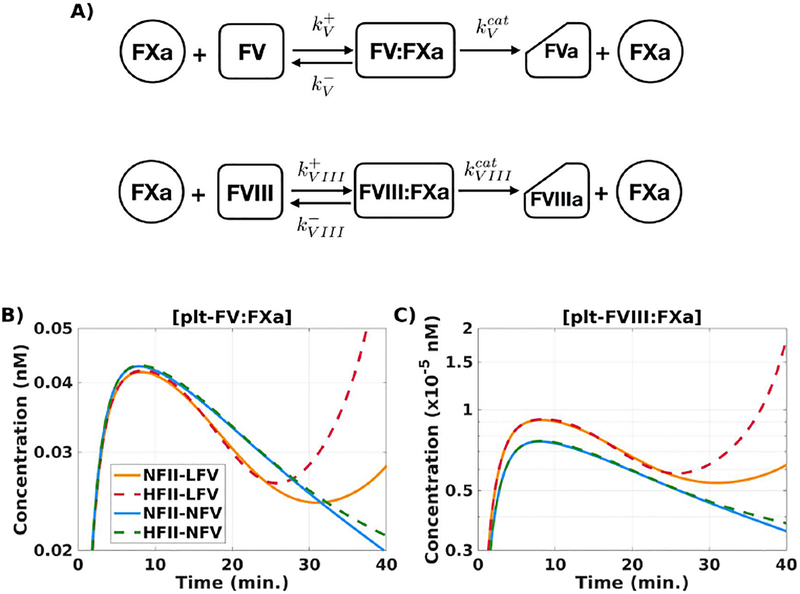
Conclusions: These results show that low-normal FV levels can enhance thrombin generation in hemophilia A. Further explorations with the mathematical model suggest a potential mechanism: lowering FV reduces competition between FV and FVIII for factor Xa (FXa) on activated platelet surfaces (APS), which enhances FVIII activation and rescues thrombin generation in FVIII-deficient blood.
Keywords: factor V; factor VIII; hemophilia A; hemorheology; hemostasis.
© 2019 International Society on Thrombosis and Haemostasis.
Conflict of interest statement
Disclosure of Conflicts of Interest
The authors declare no competing financial interests.
Figures
References
-
- Blanchette VS, Key NS, Ljung LR, et al. Definitions in hemophilia: communication from the SSC of the ISTH. J Thromb Haemost. 2014;12:1935–1939. - PubMed
-
- Carcao MD, Berg HM, Ljung R, Mancuso ME, PedNet, Rodin Study Group. Correlation between phenotype and genotype in a large unselected cohort of children with severe hemophilia A Blood. 2013;121:3946–52, S1. - PubMed
-
- Nogami K, Shima M. Phenotypic heterogeneity of hemostasis in severe hemophilia. Semin Thromb Hemost. 2015; 41:826–831. - PubMed
-
- Franchini M, Mannucci PM. Modifiers of clinical phenotype in severe congenital hemophilia. Thromb Res. 2017;156:60–64. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
