

A Consensus Molecular Classification of Muscle-invasive Bladder Cancer
- PMID: 31563503
- PMCID: PMC7690647
- DOI: 10.1016/j.eururo.2019.09.006
A Consensus Molecular Classification of Muscle-invasive Bladder Cancer
Abstract
Background: Muscle-invasive bladder cancer (MIBC) is a molecularly diverse disease with heterogeneous clinical outcomes. Several molecular classifications have been proposed, but the diversity of their subtype sets impedes their clinical application.
Objective: To achieve an international consensus on MIBC molecular subtypes that reconciles the published classification schemes.
Design, setting, and participants: We used 1750 MIBC transcriptomic profiles from 16 published datasets and two additional cohorts.
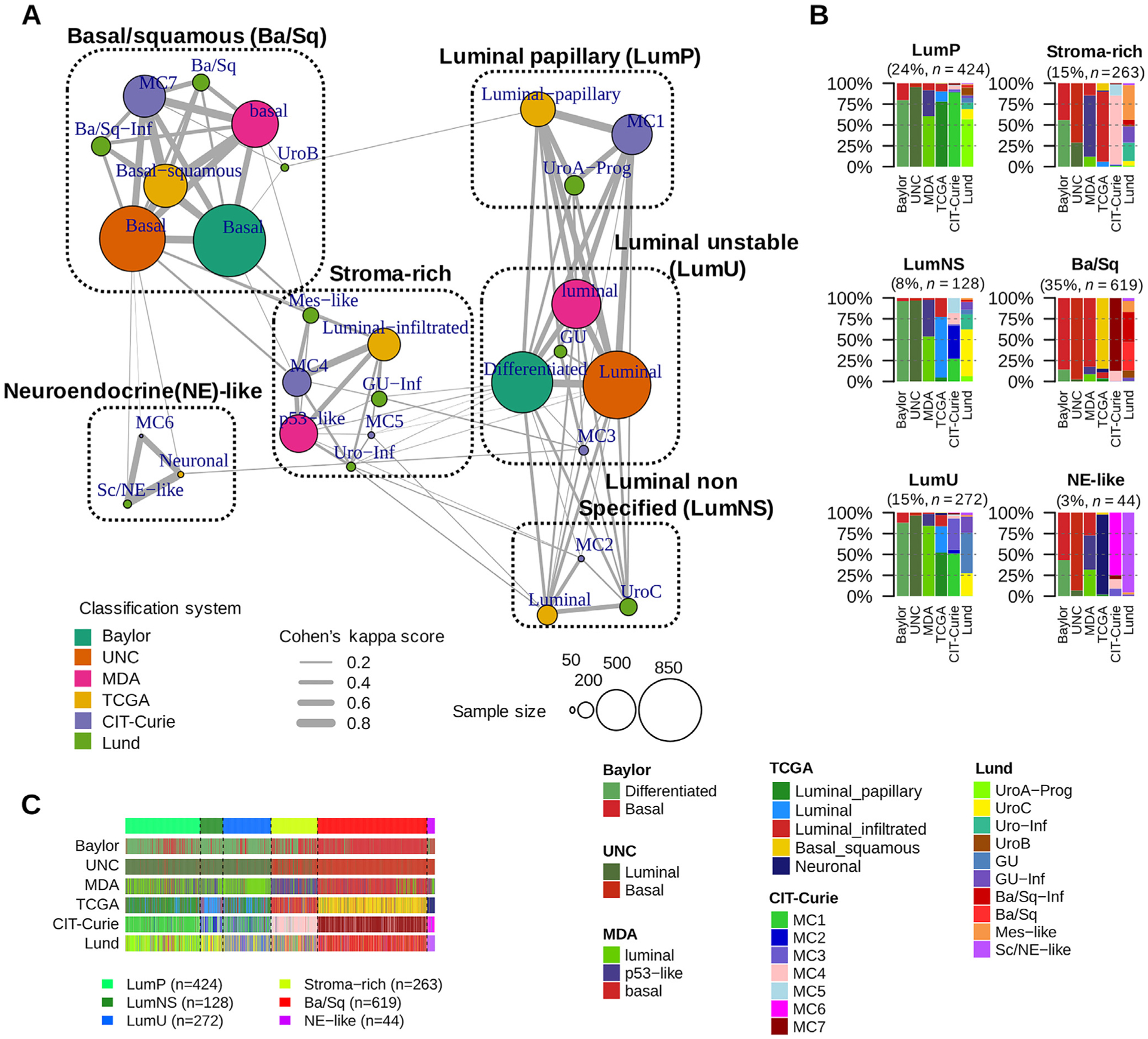
Outcome measurements and statistical analysis: We performed a network-based analysis of six independent MIBC classification systems to identify a consensus set of molecular classes. Association with survival was assessed using multivariable Cox models.
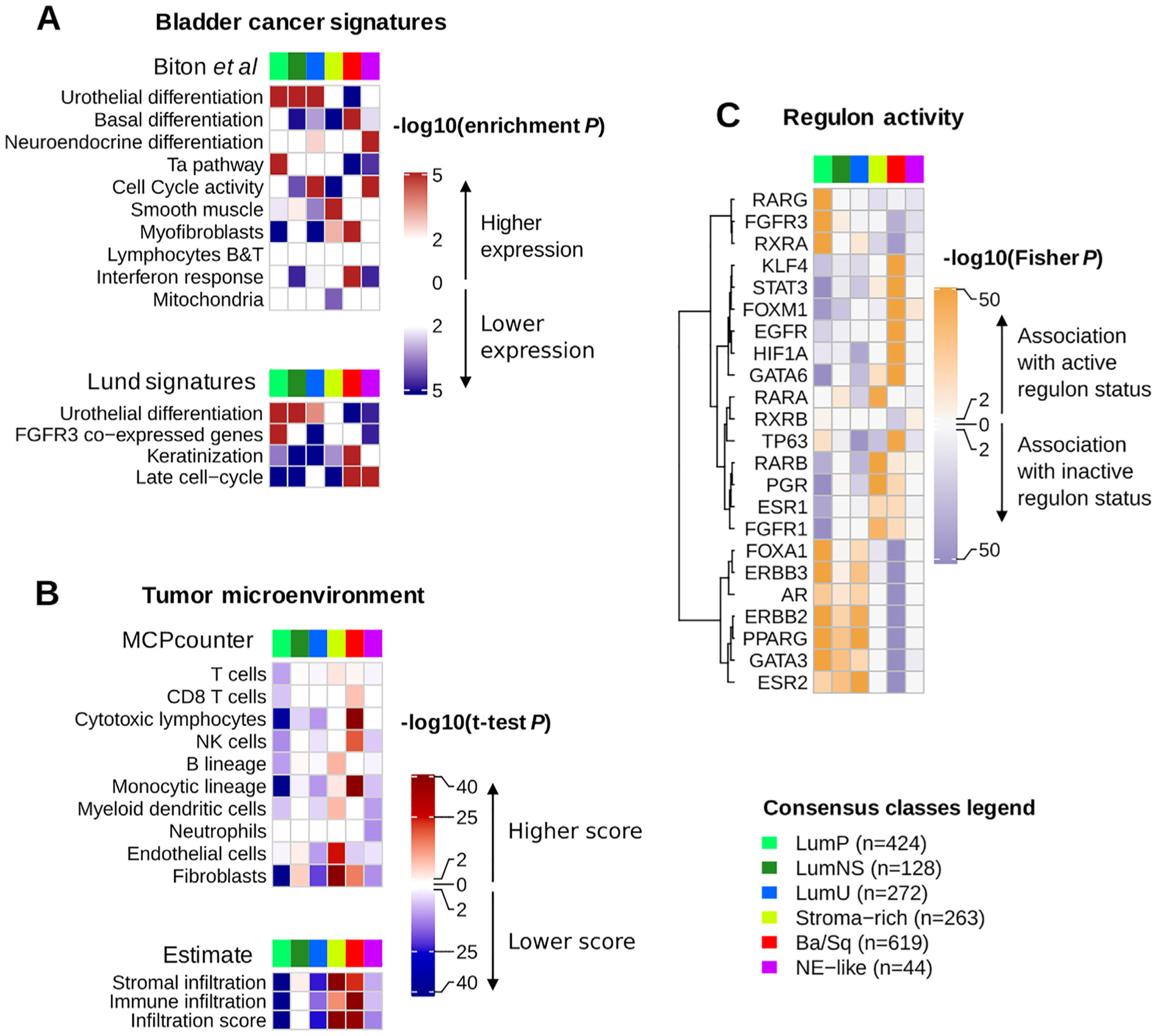
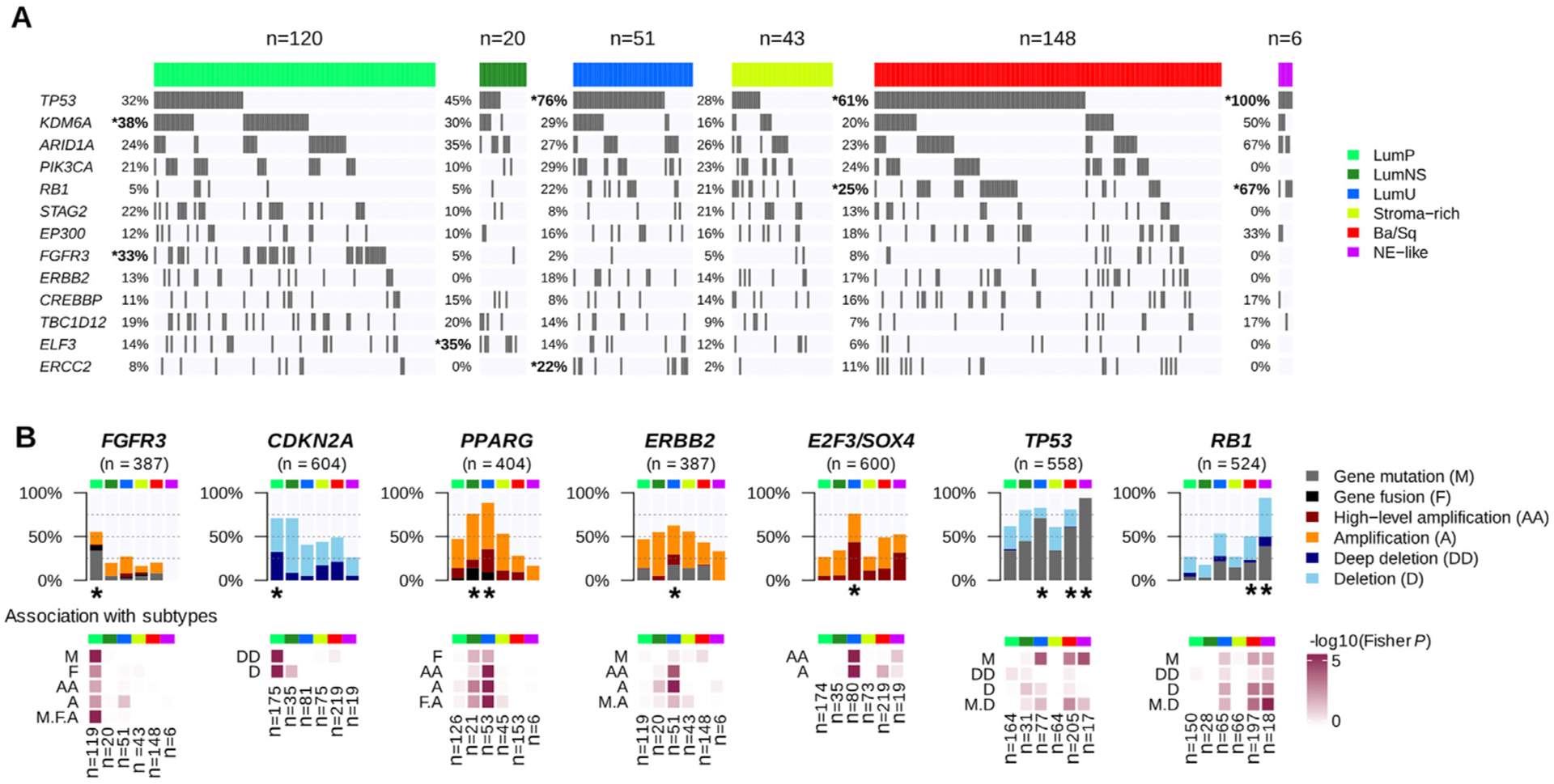
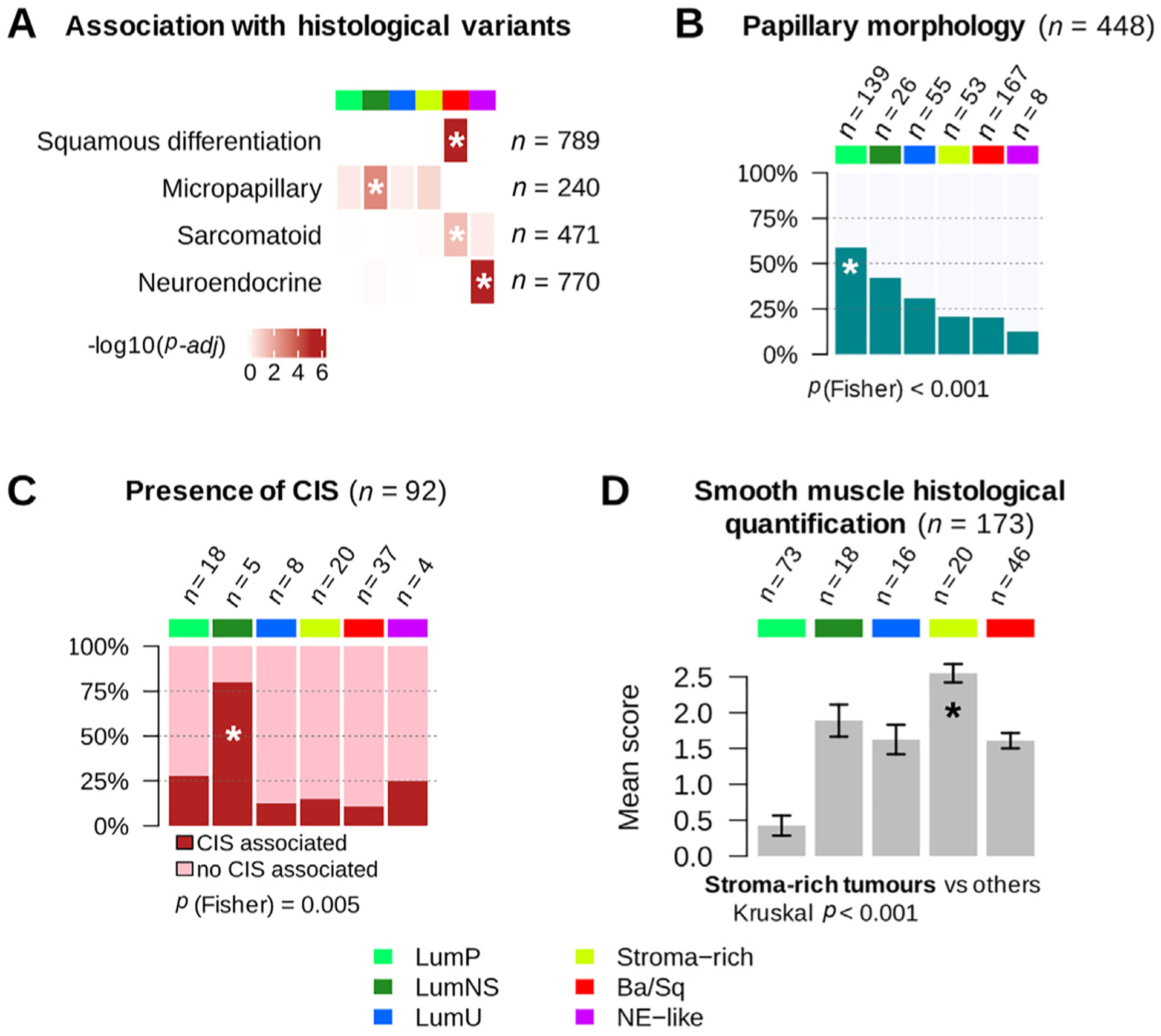
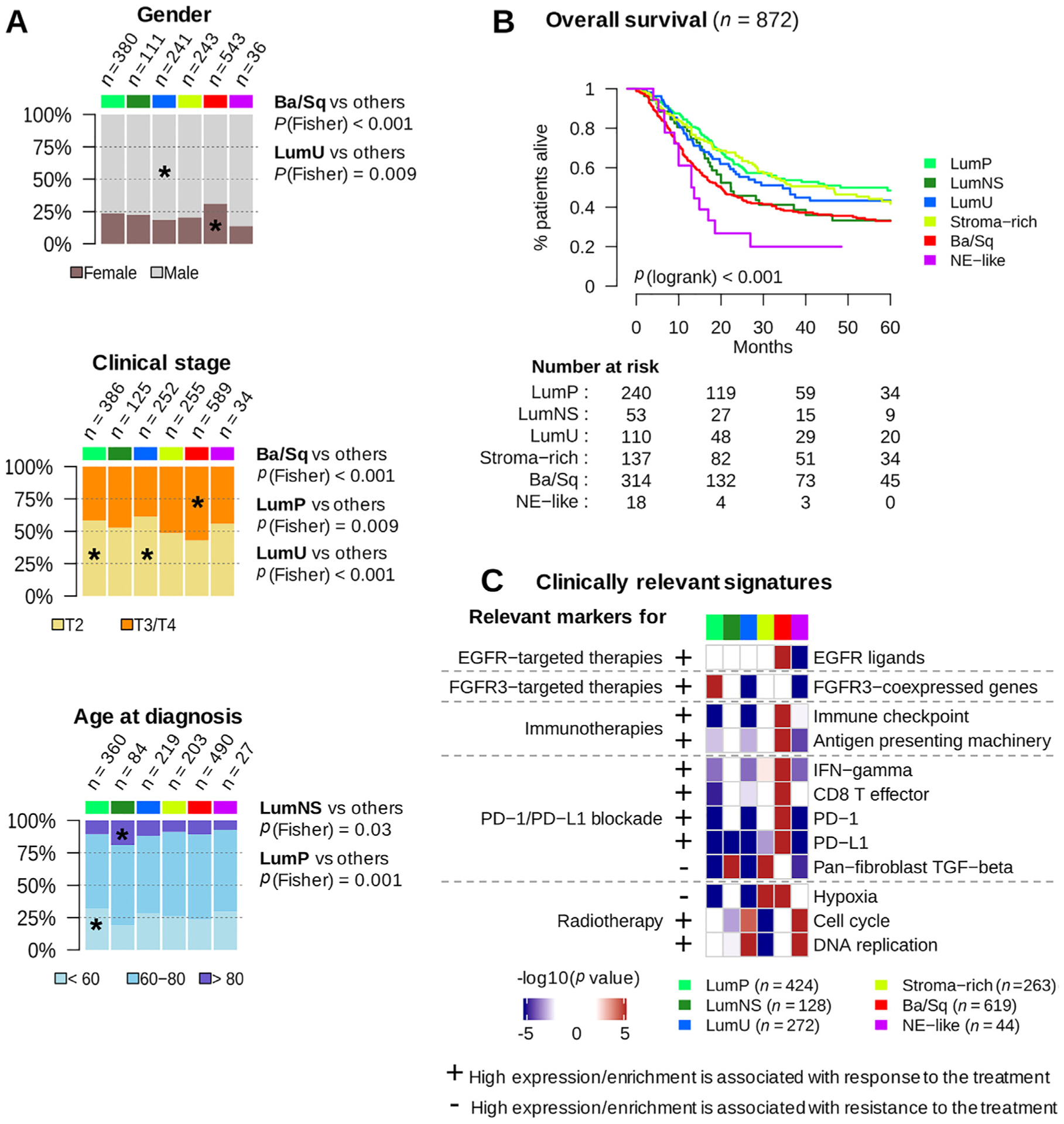
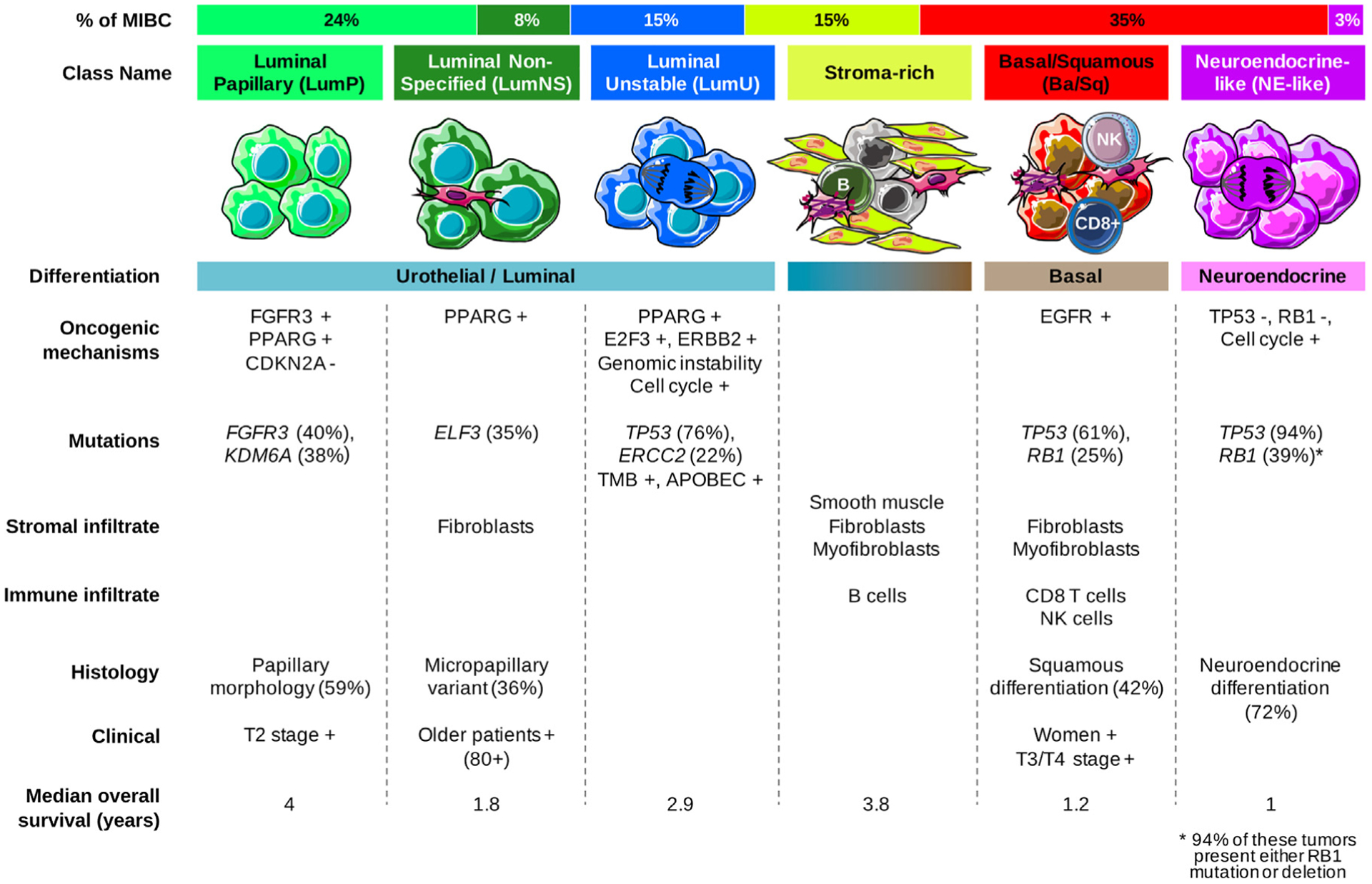
Results and limitations: We report the results of an international effort to reach a consensus on MIBC molecular subtypes. We identified a consensus set of six molecular classes: luminal papillary (24%), luminal nonspecified (8%), luminal unstable (15%), stroma-rich (15%), basal/squamous (35%), and neuroendocrine-like (3%). These consensus classes differ regarding underlying oncogenic mechanisms, infiltration by immune and stromal cells, and histological and clinical characteristics, including outcomes. We provide a single-sample classifier that assigns a consensus class label to a tumor sample's transcriptome. Limitations of the work are retrospective clinical data collection and a lack of complete information regarding patient treatment.
Conclusions: This consensus system offers a robust framework that will enable testing and validation of predictive biomarkers in future prospective clinical trials.
Patient summary: Bladder cancers are heterogeneous at the molecular level, and scientists have proposed several classifications into sets of molecular classes. While these classifications may be useful to stratify patients for prognosis or response to treatment, a consensus classification would facilitate the clinical use of molecular classes. Conducted by multidisciplinary expert teams in the field, this study proposes such a consensus and provides a tool for applying the consensus classification in the clinical setting.
Keywords: Consensus; Molecular taxonomy; Muscle-invasive bladder cancer; Transcriptomic classifier.
Copyright © 2019 The Authors. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
Consensus Genomic Subtypes of Muscle-invasive Bladder Cancer: A Step in the Right Direction but Still a Long Way To Go.Eur Urol. 2020 Apr;77(4):434-435. doi: 10.1016/j.eururo.2019.09.032. Epub 2019 Oct 24. Eur Urol. 2020. PMID: 31668376 No abstract available.
-
Re: Aurélie Kamoun, Aurélien de Reyniès, Yves Allory, et al. A Consensus Molecular Classification of Muscle-invasive Bladder Cancer. Eur Urol 2020;77:420-33: A Statement from the International Bladder Cancer Network.Eur Urol. 2020 Apr;77(4):e105-e106. doi: 10.1016/j.eururo.2019.11.011. Epub 2019 Nov 29. Eur Urol. 2020. PMID: 31787429 No abstract available.
-
Reply To Kenneth B. Yatai, Mark J. Dunning, Dennis Wang. Consensus Genomic Subtypes of Muscle-invasive Bladder Cancer: A Step in the Right Direction but Still a Long Way To Go. Eur Urol 2020;77:434-5.Eur Urol. 2020 Apr;77(4):436-438. doi: 10.1016/j.eururo.2019.12.014. Epub 2020 Feb 7. Eur Urol. 2020. PMID: 32037144 No abstract available.
-
Urological Oncology: Bladder, Penis and Urethral Cancer, and Basic Principles of Oncology.J Urol. 2021 Apr;205(4):1223-1225. doi: 10.1097/JU.0000000000001608. Epub 2021 Jan 21. J Urol. 2021. PMID: 33472376 No abstract available.
References
-
- Blaveri E, Simko JP, Korkola JE, et al. Bladder cancer outcome and subtype classification by gene expression. Clin Cancer Res 2005;11:4044–55. - PubMed
-
- Dyrskjøt L, Thykjaer T, Kruhøffer M, et al. Identifying distinct classes of bladder carcinoma using microarrays. Nat Genet 2003;33:90–6. - PubMed
-
- Lindgren D, Frigyesi A, Gudjonsson S, et al. Combined gene expression and genomic profiling define two intrinsic molecular subtypes of urothelial carcinoma and gene signatures for molecular grading and outcome. Cancer Res 2010;70:3463–72. - PubMed
-
- Sjödahl G, Lauss M, Lövgren K, et al. A molecular taxonomy for urothelial carcinoma. Clin Cancer Res 2012;18:3377–86. - PubMed
-
- Tan TZ, Rouanne M, Tan KT, Huang RY-J, Thiery J-P. Molecular subtypes of urothelial bladder cancer: results from a meta-cohort analysis of 2411 tumors. Eur Urol 2019;75:423–32. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
