

Comprehensive Prognostication in Critically Ill Pediatric Hematopoietic Cell Transplant Patients: Results from Merging the Center for International Blood and Marrow Transplant Research (CIBMTR) and Virtual Pediatric Systems (VPS) Registries
- PMID: 31563573
- PMCID: PMC6943183
- DOI: 10.1016/j.bbmt.2019.09.027
Comprehensive Prognostication in Critically Ill Pediatric Hematopoietic Cell Transplant Patients: Results from Merging the Center for International Blood and Marrow Transplant Research (CIBMTR) and Virtual Pediatric Systems (VPS) Registries
Abstract
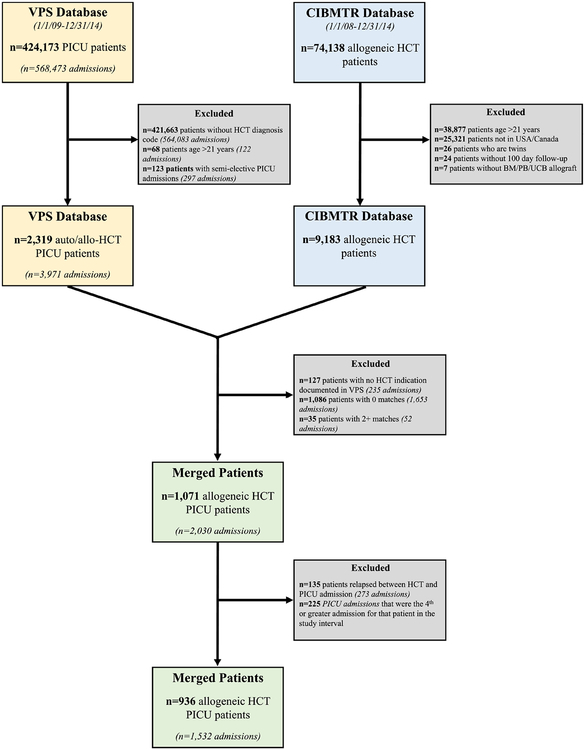
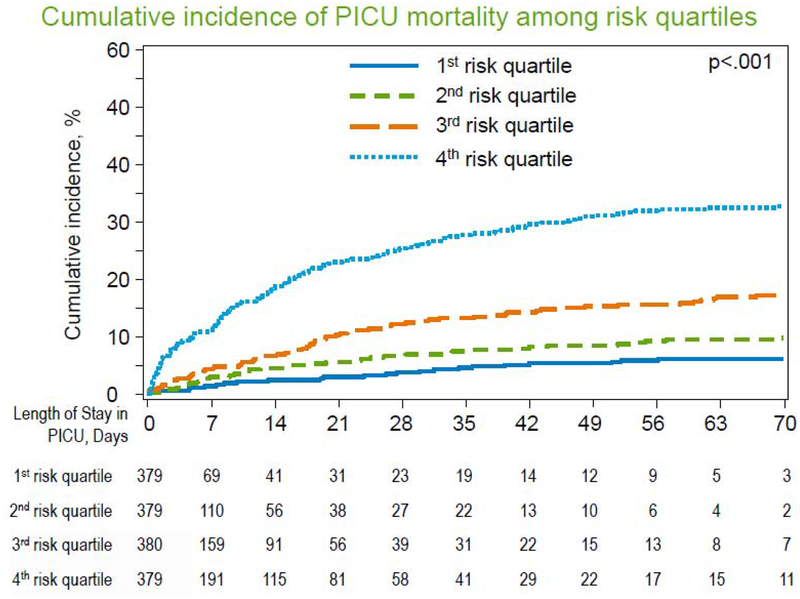
Critically ill pediatric allogeneic hematopoietic cell transplant (HCT) patients may benefit from early and aggressive interventions aimed at reversing the progression of multiorgan dysfunction. Therefore, we evaluated 25 early risk factors for pediatric intensive care unit (PICU) mortality to improve mortality prognostication. We merged the Virtual Pediatric Systems and Center for International Blood and Marrow Transplant Research databases and analyzed 936 critically ill patients ≤21 years of age who had undergone allogeneic HCT and subsequently required PICU admission between January 1, 2009, and December 31, 2014. Of 1532 PICU admissions, the overall PICU mortality rate was 17.4% (95% confidence interval [CI], 15.6% to 19.4%) but was significantly higher for patients requiring mechanical ventilation (44.0%), renal replacement therapy (56.1%), or extracorporeal life support (77.8%). Mortality estimates increased significantly the longer that patients remained in the PICU. Of 25 HCT- and PICU-specific characteristics available at or near the time of PICU admission, moderate/severe pre-HCT renal injury, pre-HCT recipient cytomegalovirus seropositivity, <100-day interval between HCT and PICU admission, HCT for underlying acute myeloid leukemia, and greater admission organ dysfunction as approximated by the Pediatric Risk of Mortality 3 score were each independently associated with PICU mortality. A multivariable model using these components identified that patients in the top quartile of risk had 3 times greater mortality than other patients (35.1% versus 11.5%, P < .001, classification accuracy 75.2%; 95% CI, 73.0% to 77.4%). These data improve our working knowledge of the factors influencing the progression of critical illness in pediatric allogeneic HCT patients. Future investigation aimed at mitigating the effect of these risk factors is warranted.
Keywords: Hematopoietic stem cell transplantation; Intensive care units; Organ dysfunction scores; Pediatric; Prognosis; Survival analysis.
Copyright © 2019 American Society for Transplantation and Cellular Therapy. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures

References
-
- D’Souza A, Fretham C. Current Uses and Outcomes of Hematopoietic Cell Transplantation (HCT): CIBMTR Summary Slides, 2017. 2017;2018.
-
- Kache S, Weiss IK, Moore TB. Changing outcomes for children requiring intensive care following hematopoietic stem cell transplantation. Pediatr.Transplant 2006;10:299–303. - PubMed
-
- Rowan CM, McArthur J, Hsing DD, et al. Acute Respiratory Failure in Pediatric Hematopoietic Cell Transplantation: A Multicenter Study. Crit.CareMed 2018;46:e967–e974. - PubMed
-
- Jacobe SJ, Hassan A, Veys P, Mok Q. Outcome of children requiring admission to an intensive care unit after bone marrow transplantation. Crit.Care Med 2003;31:1299–1305. - PubMed
-
- Duncan CN, Lehmann LE, Cheifetz IM, et al. Clinical outcomes of children receiving intensive cardiopulmonary support during hematopoietic stem cell transplant. Pediatr.Crit.Care.Med 2013;14:261–267. - PubMed
