

Gastroparesis: a turning point in understanding and treatment
- PMID: 31563877
- PMCID: PMC6874806
- DOI: 10.1136/gutjnl-2019-318712
Gastroparesis: a turning point in understanding and treatment
Abstract
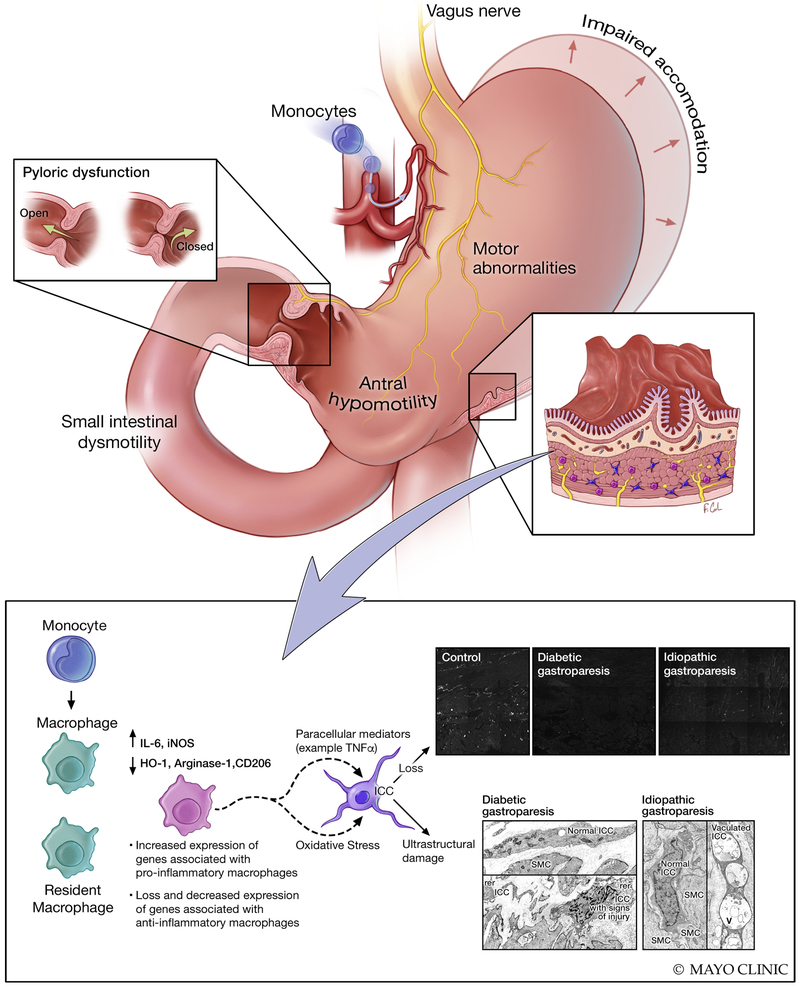
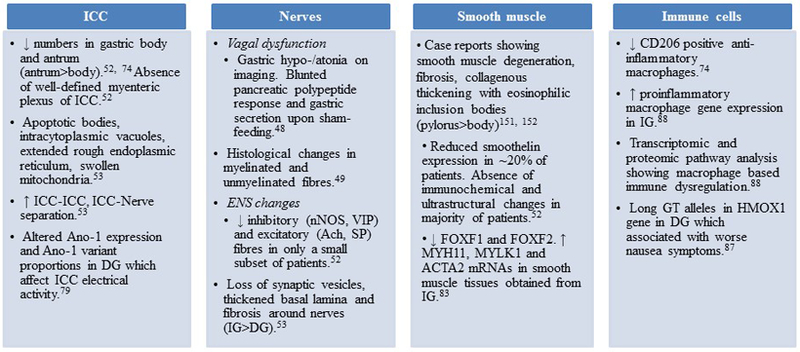
Gastroparesis is defined by delayed gastric emptying (GE) and symptoms of nausea, vomiting, bloating, postprandial fullness, early satiety and abdominal pain. Most common aetiologies include diabetes, postsurgical and postinfectious, but in many cases it is idiopathic. Clinical presentation and natural history vary by the aetiology. There is significant morbidity and healthcare utilisation associated with gastroparesis. Mechanistic studies from diabetic animal models of delayed GE as well as human full-thickness biopsies have significantly advanced our understanding of this disorder. An innate immune dysregulation and injury to the interstitial cells of Cajal and other components of the enteric nervous system through paracrine and oxidative stress mediators is likely central to the pathogenesis of gastroparesis. Scintigraphy and 13C breath testing provide the most validated assessment of GE. The stagnant gastroparesis therapeutic landscape is likely to soon see significant changes. Relatively newer treatment strategies include antiemetics (aprepitant), prokinetics (prucalopride, relamorelin) and fundic relaxants (acotiamide, buspirone). Endoscopic pyloromyotomy appears promising over the short term, especially for symptoms of nausea and vomiting. Further controlled trials and identification of the appropriate subgroup with pyloric dysfunction and assessment of long-term outcomes are essential. This review highlights the clinical presentation, diagnosis, mechanisms and treatment advancements for gastroparesis.
Keywords: GASTRIC EMPTYING; GASTROPARESIS; INTERSTITIAL CELLS OF CAJAL; MACROPHAGES; PROKINETIC AGENT.
© Author(s) (or their employer(s)) 2019. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Parkman HP, Hasler WL, Fisher RS, et al. American Gastroenterological Association medical position statement: diagnosis and treatment of gastroparesis. Gastroenterology 2004;127:1589–91. - PubMed
-
- Soykan I, Sivri B, Sarosiek I, et al. Demography, clinical characteristics, psychological and abuse profiles, treatment, and long-term follow-up of patients with gastroparesis. Dig Dis Sci 1998;43:2398–404. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources