

Impact of Hospice on Spending and Utilization Among Patients With Lung Cancer in Medicare
- PMID: 31564110
- PMCID: PMC7054142
- DOI: 10.1177/1049909119878446
Impact of Hospice on Spending and Utilization Among Patients With Lung Cancer in Medicare
Abstract
Objectives: To compare patterns and understand drivers of spending and utilization by month in the last 6 months of life between patients with lung cancer who used hospice versus those who did not.
Study design: Retrospective cohort analysis using 2009 to 2013 Medicare claims.
Methods: We used a 10% random sample of Medicare fee-for-service beneficiaries with lung cancer who died between 2010 and 2013 (43 789 beneficiaries). Patients were assigned to 2 groups depending on whether they used hospice care in the last 6 months of life. The following outcomes were constructed by month: (1) all-cause Medicare spending, (2) indicator of hospitalization, (3) indicator of emergency department (ED) visit, (4) number of part B chemotherapy claims, and (5) number of radiation therapy sessions. We used a combination of propensity score matching and regression analysis to compare outcomes between the 2 groups.
Results: Patients who used hospice had significantly lower spending in the last month of life compared to nonusers (US$16 907 vs US$26 906, P < .00). The spending differences in the last month of life between the 2 groups were largely driven by lower likelihood of hospitalization (54% vs 80%, P < .01) and ED visits (15% vs 22%, P < .01) and fewer chemotherapy (0.12 vs 0.32, P < .01) and radiation therapy sessions (0.80 vs 1.26, P < .01). During the other months in the 6-month period, spending was similar between the 2 groups.
Conclusions: Timely hospice enrollment of patients with lung cancer-the group suffering from high morbidity and mortality among patients with cancer-may lead to significant cost savings.
Keywords: Medicare; cost impact of hospice; end-of-life utilization trends; length of hospice use; lung cancer; monthly end-of-life costs.
Figures
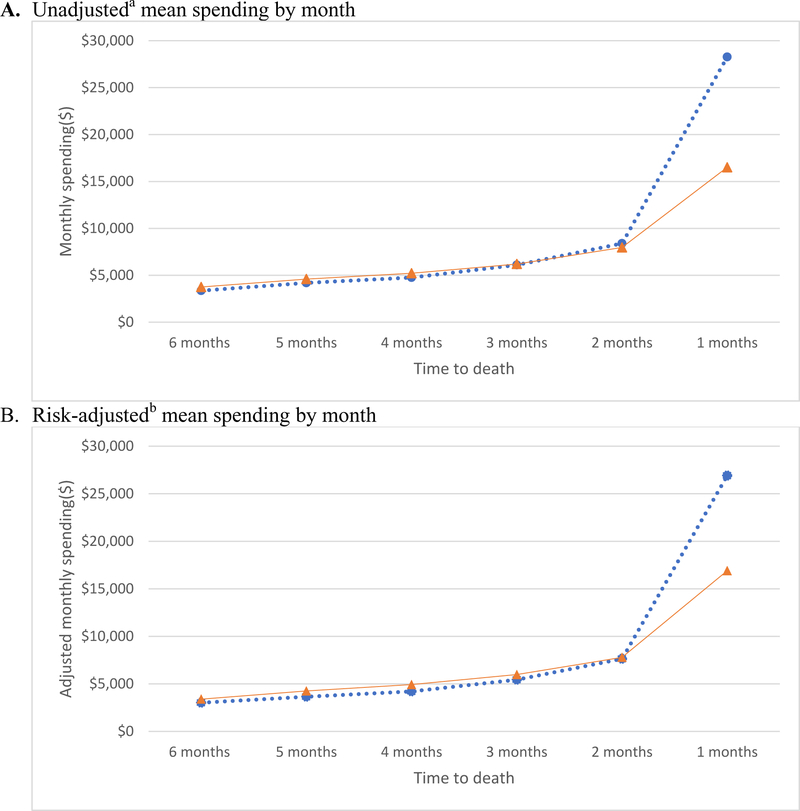
 Hospice users;
Hospice users;  Hospice non-users;
Hospice non-users;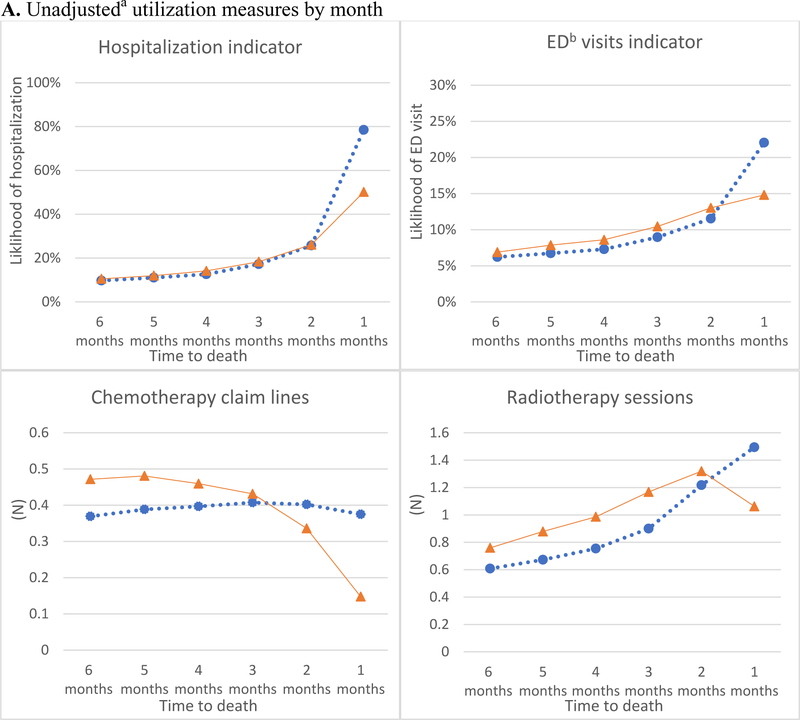
 Hospice users;
Hospice users;  Hospice non-users;
Hospice non-users;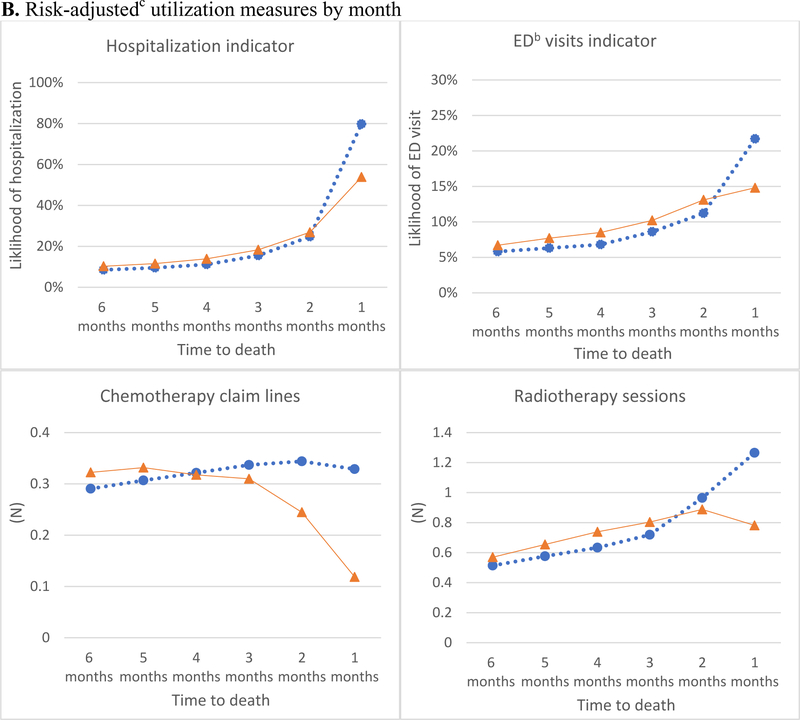 Hospice users; Hospice non-users;
Hospice users; Hospice non-users;Similar articles
-
Impact of Length of Hospice on Spending and Utilization Among Medicare Beneficiaries With Lung Cancer.Am J Hosp Palliat Care. 2020 Nov;37(11):918-924. doi: 10.1177/1049909120909304. Epub 2020 Mar 3. Am J Hosp Palliat Care. 2020. PMID: 32124636 Free PMC article.
-
Hospice Use, Hospitalization, and Medicare Spending at the End of Life.J Gerontol B Psychol Sci Soc Sci. 2016 May;71(3):569-80. doi: 10.1093/geronb/gbv109. Epub 2015 Dec 11. J Gerontol B Psychol Sci Soc Sci. 2016. PMID: 26655645
-
Longer Periods Of Hospice Service Associated With Lower End-Of-Life Spending In Regions With High Expenditures.Health Aff (Millwood). 2017 Feb 1;36(2):328-336. doi: 10.1377/hlthaff.2016.0683. Health Aff (Millwood). 2017. PMID: 28167723 Free PMC article.
-
Race, Any Cancer, Income, or Cognitive Function: What Inf luences Hospice or Aggressive Services Use at the End of Life Among Community-Dwelling Medicare Beneficiaries?Am J Hosp Palliat Care. 2016 Jul;33(6):537-45. doi: 10.1177/1049909115574263. Epub 2015 Mar 9. Am J Hosp Palliat Care. 2016. PMID: 25753184 Free PMC article. Review. No abstract available.
-
Primary Care Spending in Medicare Fee-for-Service: An Illustrative Analysis Using Alternative Definitions of Primary Care: Issue Brief [Internet].Washington (DC): Office of the Assistant Secretary for Planning and Evaluation (ASPE); 2024 Mar 5. Report No.: HP-2024-05. Washington (DC): Office of the Assistant Secretary for Planning and Evaluation (ASPE); 2024 Mar 5. Report No.: HP-2024-05. PMID: 39913652 Free Books & Documents. Review.
Cited by
-
Impact of next-generation sequencing vs polymerase chain reaction testing on payer costs and clinical outcomes throughout the treatment journeys of patients with metastatic non-small cell lung cancer.J Manag Care Spec Pharm. 2024 Dec;30(12):1467-1478. doi: 10.18553/jmcp.2024.24137. Epub 2024 Sep 11. J Manag Care Spec Pharm. 2024. PMID: 39259000 Free PMC article.
-
Impact of Length of Hospice on Spending and Utilization Among Medicare Beneficiaries With Lung Cancer.Am J Hosp Palliat Care. 2020 Nov;37(11):918-924. doi: 10.1177/1049909120909304. Epub 2020 Mar 3. Am J Hosp Palliat Care. 2020. PMID: 32124636 Free PMC article.
References
-
- Howlader N, Noone AM, Krapcho M, et al. SEER Cancer Statistics Review, 1975–2014 National Cancer Institute. Bethesda, MD, https://seer.cancer.gov/csr/1975_2014/, based on November 2016 SEER data submission, posted to the SEER web site, April 2017.
-
- Temel JS, Greer JA, Muzikansky A, et al. Early Palliative Care for Patients with Metastatic Non–Small-Cell Lung Cancer. The New England Journal of Medicine. 2010;363:733–742. - PubMed
-
- Robinson BE, Pham H. Cost-effectiveness of hospice care. Clinics in geriatric medicine. 1996;12:417. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
