

What do Workplace Wellness Programs do? Evidence from the Illinois Workplace Wellness Study
- PMID: 31564754
- PMCID: PMC6756192
- DOI: 10.1093/qje/qjz023
What do Workplace Wellness Programs do? Evidence from the Illinois Workplace Wellness Study
Abstract
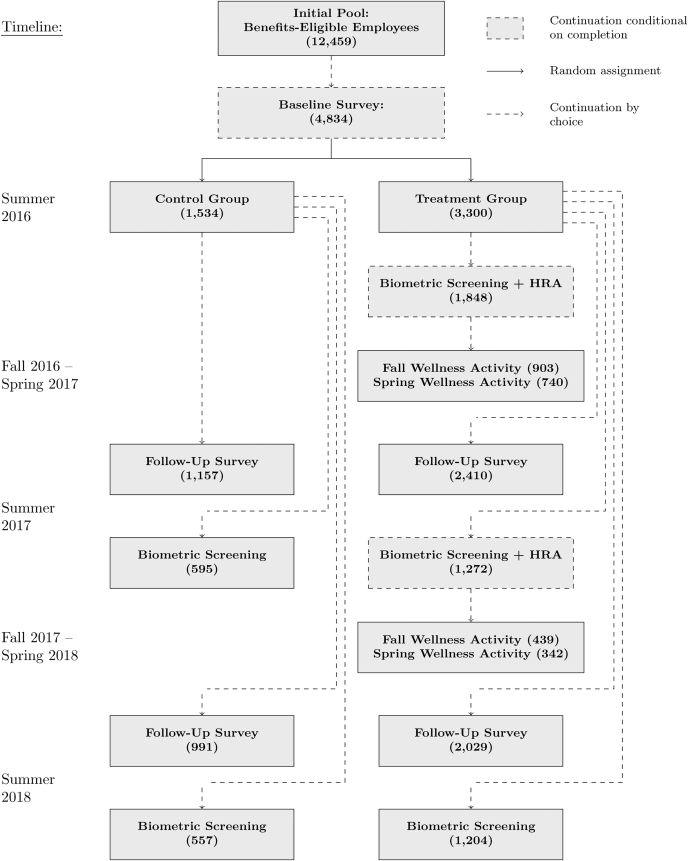
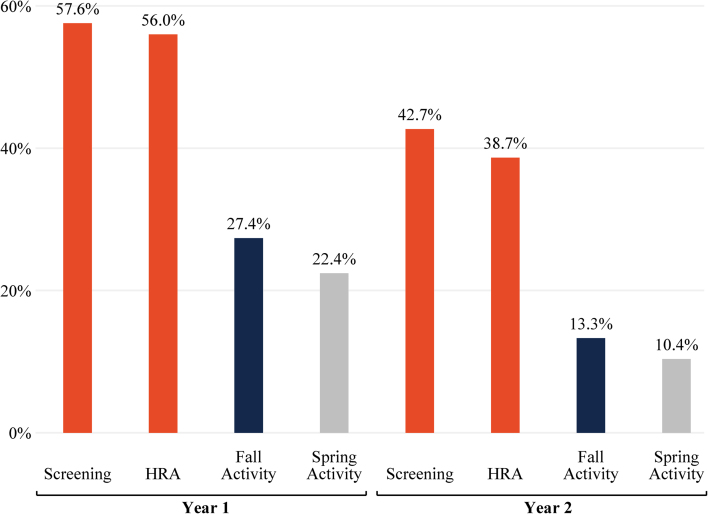
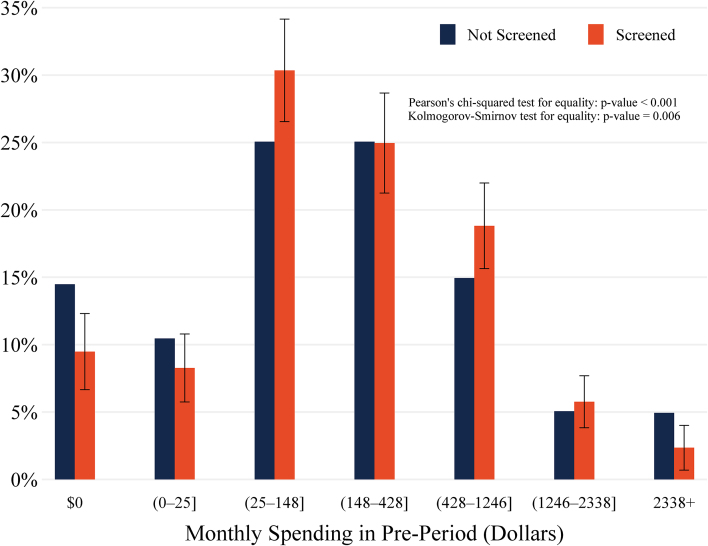
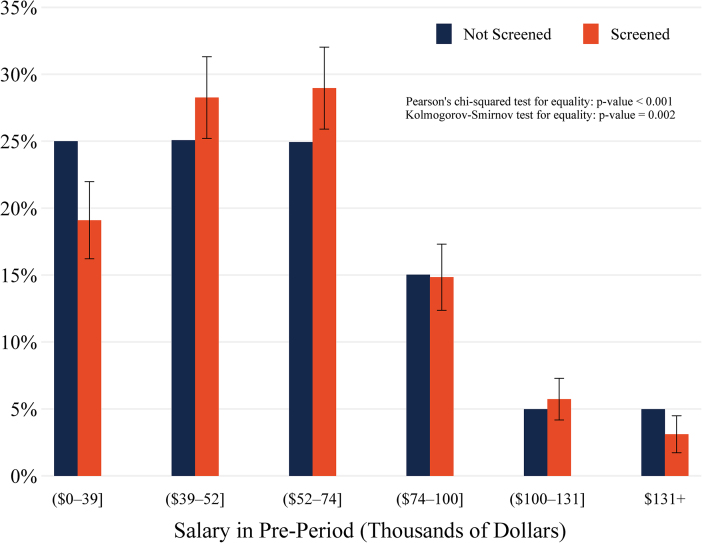
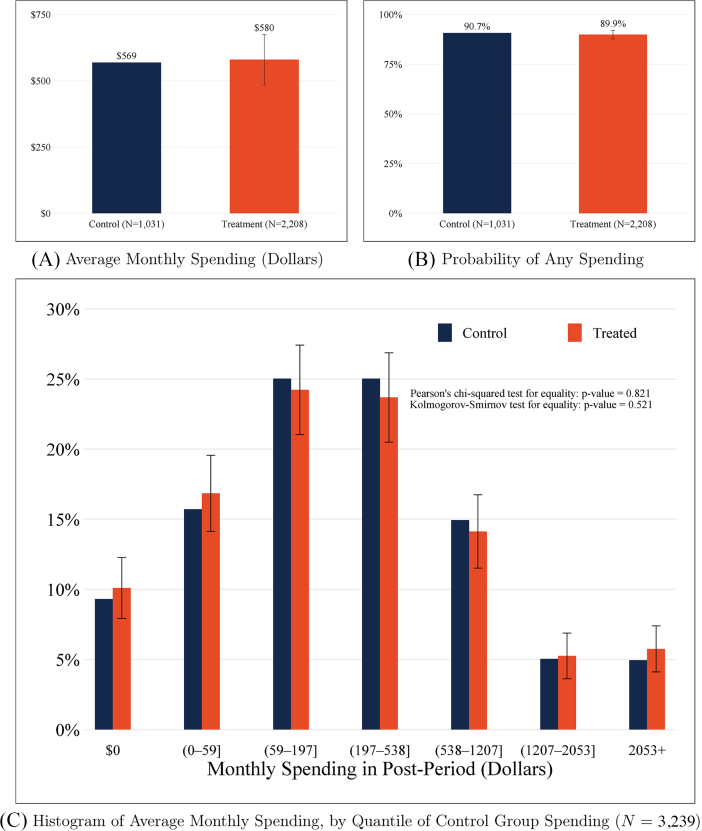
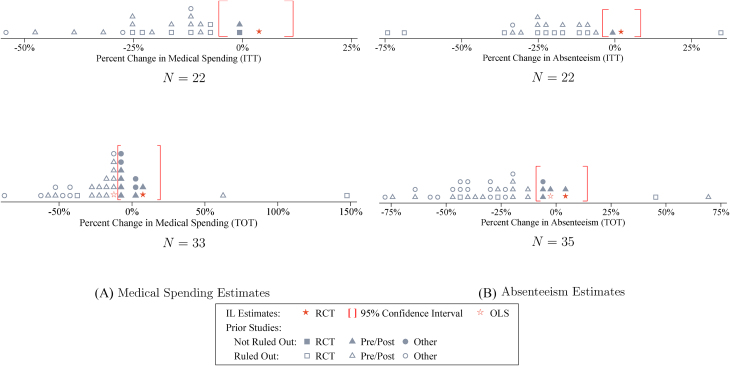
Workplace wellness programs cover over 50 million U.S. workers and are intended to reduce medical spending, increase productivity, and improve well-being. Yet limited evidence exists to support these claims. We designed and implemented a comprehensive workplace wellness program for a large employer and randomly assigned program eligibility and financial incentives at the individual level for nearly 5,000 employees. We find strong patterns of selection: during the year prior to the intervention, program participants had lower medical expenditures and healthier behaviors than nonparticipants. The program persistently increased health screening rates, but we do not find significant causal effects of treatment on total medical expenditures, other health behaviors, employee productivity, or self-reported health status after more than two years. Our 95% confidence intervals rule out 84% of previous estimates on medical spending and absenteeism.
© The Author(s) 2019. Published by Oxford University Press on behalf of President and Fellows of Harvard College.
Figures
Comment in
-
Commentary on the Study: "What Do Workplace Wellness Programs Do? Evidence From the Illinois Workplace Wellness Study".Am J Health Promot. 2020 May;34(4):440-444. doi: 10.1177/0890117120906664. Epub 2020 Feb 20. Am J Health Promot. 2020. PMID: 32077304
-
Reply to Dr Goetzel.Am J Health Promot. 2020 May;34(4):445. doi: 10.1177/0890117120906661. Epub 2020 Feb 24. Am J Health Promot. 2020. PMID: 32088971 No abstract available.
References
-
- Abadie Alberto, Athey Susan, Imbens Guido, Wooldridge Jeffrey, “When Should You Adjust Standard Errors for Clustering?,” NBER Working Paper no. 24003, 2017.
-
- Abraham Jean, White Katie M., “Tracking the Changing Landscape of Corporate Wellness Companies,” Health Affairs, 36 (2017), 222–228. - PubMed
-
- Aldana Steven G., “Financial Impact of Health Promotion Programs: A Comprehensive Review of the Literature,” American Journal of Health Promotion, 15 (2001), 296–320. - PubMed
-
- Andrews Isaiah, Kasy Maximilian, “Identification of and Correction for Publication Bias,” American Economic Review, 109 (2019), 2766–2794.
-
- Baicker Katherine, Cutler David, Song Zirui, “Workplace Wellness Programs Can Generate Savings,” Health Affairs, 29 (2010), 304–311. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical