

Cytological and Wet Mount Microscopic Observations Made in Urine of Schistosoma haematobium-Infected Children: Hint of the Implication in Bladder Cancer
- PMID: 31565106
- PMCID: PMC6745107
- DOI: 10.1155/2019/7912186
Cytological and Wet Mount Microscopic Observations Made in Urine of Schistosoma haematobium-Infected Children: Hint of the Implication in Bladder Cancer
Abstract
Background: Schistosomiasis is the second major human parasitic disease next to malaria, in terms of socioeconomic and public health consequences, especially in sub-Saharan Africa. Schistosoma haematobium (S. haematobium) is a trematode and one of the species of Schistosoma that cause urogenital schistosomiasis (urinary schistosomiasis). Although the knowledge of this disease has improved over the years, there are still endemic areas, with most of the reported cases in Africa, including Ghana. Not much has been done in Ghana to investigate cytological abnormalities in individuals within endemic communities, although there are epidemiologic evidences linking S. haematobium infection with carcinoma of the bladder.
Aim: The aim of this study was to identify microscopic and cytological abnormalities in the urine deposits of S. haematobium-infected children.
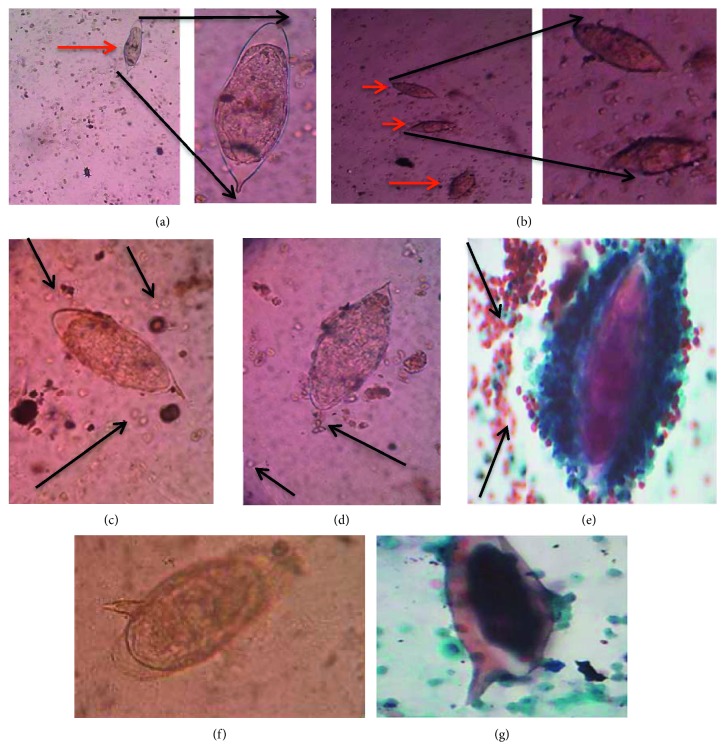
Methodology: Three hundred and sixty-seven (367) urine samples were collected from school children in Zenu and Weija communities. All the samples were examined microscopically for the presence of S. haematobium eggs, after which the infected samples and controls were processed for cytological investigation.
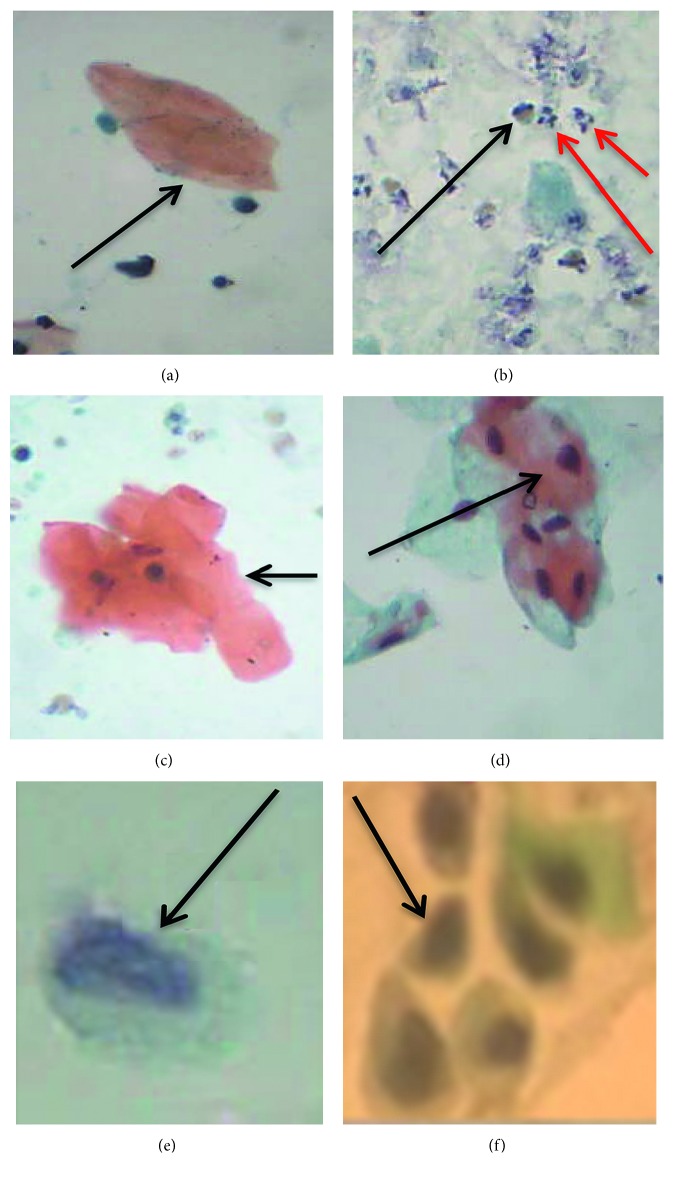
Results: S. haematobium ova were present in 66 (18.0%) out of the 367 urine samples. Inflammatory cells (82%, 54/66), hyperkeratosis (47%, 31/66), and squamous cell metaplasia (24%, 16/66) were the main observations made during the cytological examination of the S. haematobium-infected urine samples.
Conclusion: Cytological abnormalities in S. haematobium-infected children may play an important role in the severity of the disease, leading to the possible development of bladder cancer in later years, if early attention is not given. Therefore, routine cytological screening for urogenital schistosomiasis patients (especially children) at hospitals in S. haematobium-endemic locations is recommended.
Copyright © 2019 Patience B. Tetteh-Quarcoo et al.
Conflict of interest statement
The authors declare that there are no conflicts of interest regarding the publication of this article.
Figures
Similar articles
-
Dynamics in Morbidity Markers and Cytological Observations Made in Urine of Schistosoma haematobium-Infected Children: Pre- and Post-Praziquantel Treatment in an Endemic Setting.Med Sci (Basel). 2022 Feb 17;10(1):14. doi: 10.3390/medsci10010014. Med Sci (Basel). 2022. PMID: 35225947 Free PMC article.
-
Concurrent Schistosoma mansoni and Schistosoma haematobium infections in a peri-urban community along the Weija dam in Ghana: A wake up call for effective National Control Programme.Acta Trop. 2019 Nov;199:105116. doi: 10.1016/j.actatropica.2019.105116. Epub 2019 Jul 26. Acta Trop. 2019. PMID: 31356786
-
Detection of cytological abnormalities in urothelial cells from individuals previously exposed or currently infected with Schistosoma haematobium.PLoS One. 2023 Mar 30;18(3):e0278202. doi: 10.1371/journal.pone.0278202. eCollection 2023. PLoS One. 2023. PMID: 36996097 Free PMC article.
-
Review of Recent Prevalence of Urogenital Schistosomiasis in Sub-Saharan Africa and Diagnostic Challenges in the Field Setting.Life (Basel). 2023 Jul 31;13(8):1670. doi: 10.3390/life13081670. Life (Basel). 2023. PMID: 37629527 Free PMC article. Review.
-
Female genital schistosomiasis as a risk-factor for the transmission of HIV.Int J STD AIDS. 1994 Sep-Oct;5(5):368-72. doi: 10.1177/095646249400500517. Int J STD AIDS. 1994. PMID: 7819359 Review.
Cited by
-
Programmed Cell Death-Ligand-1 expression in Bladder Schistosomal Squamous Cell Carcinoma - There's room for Immune Checkpoint Blockage?.Front Immunol. 2022 Sep 2;13:955000. doi: 10.3389/fimmu.2022.955000. eCollection 2022. Front Immunol. 2022. PMID: 36148227 Free PMC article. Review.
-
Human microbiomes in cancer development and therapy.MedComm (2020). 2023 Feb 26;4(2):e221. doi: 10.1002/mco2.221. eCollection 2023 Apr. MedComm (2020). 2023. PMID: 36860568 Free PMC article. Review.
-
Dynamics in Morbidity Markers and Cytological Observations Made in Urine of Schistosoma haematobium-Infected Children: Pre- and Post-Praziquantel Treatment in an Endemic Setting.Med Sci (Basel). 2022 Feb 17;10(1):14. doi: 10.3390/medsci10010014. Med Sci (Basel). 2022. PMID: 35225947 Free PMC article.
References
-
- WHO. Weekly Epidemiological Record. Geneva, Switzerland: WHO; 2006. Schistosomiasis and soil-transmitted helminthiases: number of people treated in 2016. - PubMed
-
- Aboagye I. F., Edoh D. Investigation of the risk of infection of urinary schistosomiasis at Mahem and Galilea communities in the Greater Accra region of Ghana. West African Journal of Applied Ecology. 2009;15(1) doi: 10.4314/wajae.v15i1.49426. - DOI
-
- Anto F., Asoala V., Anyorigiya T., et al. Simultaneous administration of praziquantel, ivermectin and albendazole, in a community in rural northern Ghana endemic for schistosomiasis, onchocerciasis and lymphatic filariasis. Tropical Medicine & International Health. 2011;16(9):1112–1119. doi: 10.1111/j.1365-3156.2011.02814.x. - DOI - PubMed
LinkOut - more resources
Full Text Sources
