

Early prediction of noninvasive ventilation failure in COPD patients: derivation, internal validation, and external validation of a simple risk score
- PMID: 31565779
- PMCID: PMC6766459
- DOI: 10.1186/s13613-019-0585-9
Early prediction of noninvasive ventilation failure in COPD patients: derivation, internal validation, and external validation of a simple risk score
Abstract
Background: Early identification of noninvasive ventilation (NIV) failure is a promising strategy for reducing mortality in chronic obstructive pulmonary disease (COPD) patients. However, a risk-scoring system is lacking.
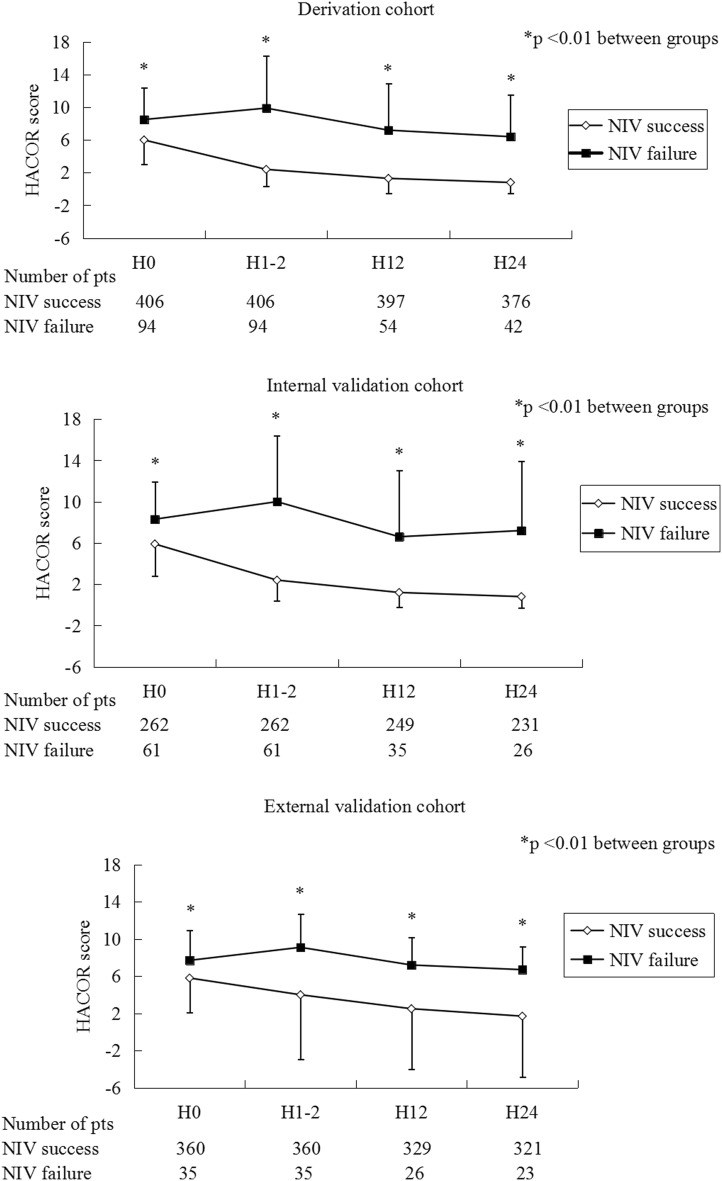
Methods: To develop a scale to predict NIV failure, 500 COPD patients were enrolled in a derivation cohort. Heart rate, acidosis (assessed by pH), consciousness (assessed by Glasgow coma score), oxygenation, and respiratory rate (HACOR) were entered into the scoring system. Another two groups of 323 and 395 patients were enrolled to internally and externally validate the scale, respectively. NIV failure was defined as intubation or death during NIV.
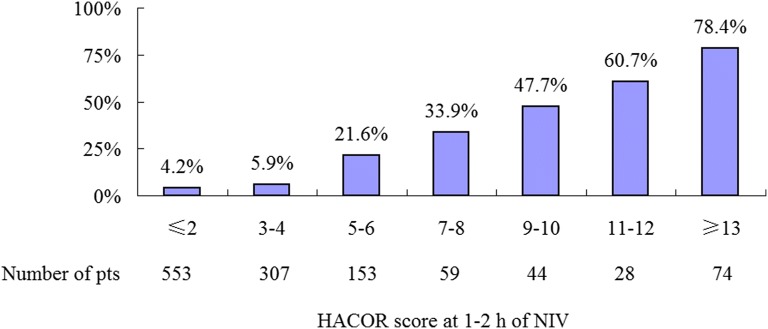
Results: Using HACOR score collected at 1-2 h of NIV to predict NIV failure, the area under the receiver operating characteristic curves (AUC) was 0.90, 0.89, and 0.71 for the derivation, internal-validation, and external-validation cohorts, respectively. For the prediction of early NIV failure in these three cohorts, the AUC was 0.91, 0.96, and 0.83, respectively. In all patients with HACOR score > 5, the NIV failure rate was 50.2%. In these patients, early intubation (< 48 h) was associated with decreased hospital mortality (unadjusted odds ratio = 0.15, 95% confidence interval 0.05-0.39, p < 0.01).
Conclusions: HACOR scores exhibited good predictive power for NIV failure in COPD patients, particularly for the prediction of early NIV failure (< 48 h). In high-risk patients, early intubation was associated with decreased hospital mortality.
Keywords: COPD exacerbations; Critical care; Noninvasive ventilation.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Appendini L, Patessio A, Zanaboni S, Carone M, Gukov B, Donner CF, Rossi A. Physiologic effects of positive end-expiratory pressure and mask pressure support during exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1994;149:1069–1076. doi: 10.1164/ajrccm.149.5.8173743. - DOI - PubMed
-
- Ram FS, Picot J, Lightowler J, Wedzicha JA. Non-invasive positive pressure ventilation for treatment of respiratory failure due to exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2004:CD004104. - PubMed
-
- Wedzicha JAEC-C, Miravitlles M, Hurst JR, Calverley PM, Albert RK, Anzueto A, Criner GJ, Papi A, Rabe KF, Rigau D, et al. Management of COPD exacerbations: a European Respiratory Society/American Thoracic Society guideline. Eur Respir J. 2017;49:1600791. doi: 10.1183/13993003.00791-2016. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
