

Suitable Use of Injectable Agents to Overcome Hypoglycemia Risk, Barriers, and Clinical Inertia in Community-Dwelling Older Adults with Type 2 Diabetes Mellitus
- PMID: 31565780
- PMCID: PMC7481154
- DOI: 10.1007/s40266-019-00706-4
Suitable Use of Injectable Agents to Overcome Hypoglycemia Risk, Barriers, and Clinical Inertia in Community-Dwelling Older Adults with Type 2 Diabetes Mellitus
Erratum in
-
Correction to: Suitable Use of Injectable Agents to Overcome Hypoglycemia Risk, Barriers, and Clinical Inertia in Community-Dwelling Older Adults with Type 2 Diabetes Mellitus.Drugs Aging. 2020 Oct;37(10):777. doi: 10.1007/s40266-020-00795-6. Drugs Aging. 2020. PMID: 32909196 Free PMC article.
Abstract
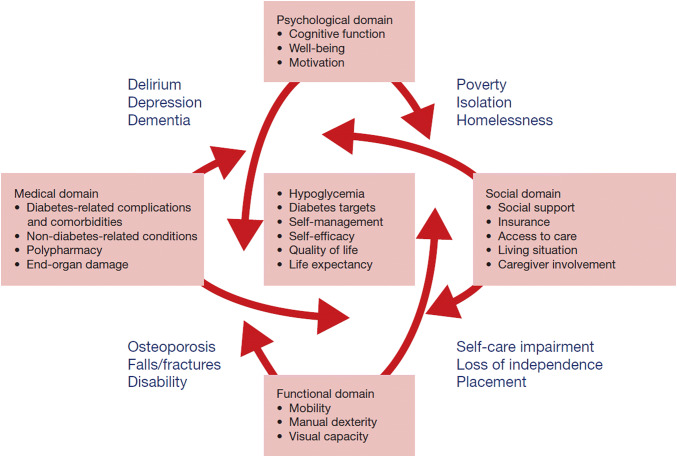
The management of type 2 diabetes mellitus in older adults requires a comprehensive understanding of the relationship between the disease (medical) and the functional, psychological/cognitive, and social geriatric domains, to individualize both glycemic targets and therapeutic approaches. Prevention of hypoglycemia is a major priority that should be addressed as soon as its presence or risk is detected, adjusting the target and therapeutics accordingly. Nonetheless, treatment intensification should not be neglected when applicable, consistent with recommendations from organizations such as the American Geriatrics Society and the American Diabetes Association, to reduce not only long-term macrovascular and microvascular complications (individualization), but also short-term complications from hyperglycemia (polyuria, volume depletion, urinary incontinence). Such complications can negatively impact the physical and cognitive function of older adults, worsen their quality of life, and additionally affect their families and society. We emphasize individualization, utilizing the multiple classes of antihyperglycemic agents available. Metformin remains as first-line therapy, and additional agents offer advantages and disadvantages that ought to be considered when developing a patient-centric plan of care. For selected cases, injectable therapies such as long-acting basal insulin analogs and glucagon-like peptide-1 receptor agonists can offer advantages to counter hypoglycemia risk, patient-related barriers, and clinical inertia. Furthermore, some injectable agents could potentially simplify regimens while providing safe and effective glycemic control. In this review, we discuss the use of injectable therapies for selected community-dwelling older adults, barriers to transition to injectable therapy, and measures aimed at removing these barriers and assisting physicians and their teams to transition older patients to injectable therapies when appropriate.
Conflict of interest statement
Willy M. Valencia and Ana M. Palacio have nothing to declare. Hermes J. Florez is a consultant (in a scientific advisory capacity) for the SENIOR study.
Figures
References
-
- Valencia WM, Florez H. Pharmacological treatment of diabetes in older people. Diabetes Obes Metab. 2014;16:1192–1203. - PubMed
-
- Valencia WM, Botros D, Vera-Nunez M, Dang S. Diabetes treatment in the elderly: incorporating geriatrics, technology, and functional medicine. Curr Diab Rep. 2018;18:95. - PubMed
-
- Sinclair AJ, Abdelhafiz AH, Forbes A, Munshi M. Evidence-based diabetes care for older people with Type 2 diabetes: a critical review. Diabet Med. 2019;36(4):399–413. - PubMed
-
- Florez HJ. Glycaemic control and glycaemic variability in older people with diabetes. Lancet Diabetes Endocrinol. 2018;6(6):433–435. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
